
ISBN 978-963-414-759-6
ORCID: https://orcid.org/0000-0003-2686-1055
Publishing Director: Ádám Gyenes
L’Harmattan Kiadó
Kossuth Lajos utca 14-16.
H-1053 Budapest
L’Harmattan France
5-7 rue de l’Ecole Polytechnique
75005 Paris
© Tamás Rácz MD, PhD, MSc, 2021
© L’Harmattan Kiadó, 2021
All rights reserved. The work and its parts are copyrighted. Any use beyond what is permitted by law is subject to the prior written consent of the publisher.
Acknowledgement: Adrien Rácz MD, Zoltán Mucsi, Kinga Budai, Boldizsár Kovács, Tamás L. Rácz
Competing Interest Statement: The author has declared no competing interest.
Funding Statement: No external funding was received.
Open Accessible:
| English: | https://media.harmattan.hu/webbook/else/ENG |
| Hungarian: | https://media.harmattan.hu/webbook/else/HUN |
Illustration in the cover page: By Susan Heavey © REUTERS/Shannon Stapleton, funeral for COVID-19 patient in Chicago, Illinois, US.
Keywords: SARS-CoV-2; COVID-19; Vulnerable Population (VP); Herd Immunity (HI); Vaccination; Non-Pharmaceutical Intervention (NPI); Socio-economic; Compliance; Immunosenescence; NK cells innate immunit response; T cell adaptive immunity response; Contagiousness; Mutation; Mortality; ELSE
ABSTRACT
1. INTRODUCTION
1.1. There have been extremely few deaths in children with SARS-CoV-2 infection and also the incidence of post-COVID-19 syndrome
1.2. Children do not substantially transmit SARS-CoV-2 infection, do not participate substantially in the transmission of COVID-19.
1.3. The importance of the protective function of the mucosa in children.
1.4. The role of innate (NK cells), non-specific immune response in COVID-19
1.5. Importance of the upper respiratory tract mucosal vaccination
1.6. Genetic modification, Antibody-Dependent Enhancement (ADE), autoimmune reaction
1.7. Factors influencing herd immunity and its unlikely development.
1.7.1. Current vaccines are questionable about preventing transmission
1.7.2. New variants increase the level of herd immunity
1.7.3. Current parenteral vaccines contribute to the development of new variants
1.7.4. Vaccine allocation is uneven
1.8. Even with high levels of herd immunity, the Elderly Vulnerable Population can only be protected either by biological vaccination or by measures recommended for those over 60 years of age, including physical isolation
1.9. Immunosenescence in the elderly
1.10. Persistent immunity acquired through natural infection
1.11. Further evidence for the development and persistence of persistent humoral and cellular immunity
1.12. Preventive intensive care alone costs more than providing physical protection (2.7.1.)
1.13. A vicious circle that persists despite the rise of mass vaccinations
1.14. Endpoints in clinical trials of recently approved and under development vaccines have not examined efficacy in mortality, and therefore new vaccines have not been shown to be effective in the mortality of the elderly
1.15. New approach, feasibility = ELSE study
1.15.1. The VP identification:
1.15.2. Reality vs. skepticism concerning the possibility of the isolation
1.15.3. Moral basis of Vulnerable Population isolation
1.16. Responsibilities of decision makers and authorities
1.17. International adaptation of ELSE
2. METHOD
2.1. The ELSE EM
2.1.1. The compartment model
2.1.2. Mathematical description of the compartment model
2.1.3. The epidemiological parameters
2.1.4. The Explanation of Control Panel (CP) and the Interactive Graphical User Interface (GUI) of the ELSE-EM model.
2.2. The role of IFR, ICU mortality rate, R0-Re in the selection criteria of ELSE VP.
2.2.1. Assessing the IFR and R0
2.2.2. The mortality rate in the present availability or the absence of ICU
2.3. The role of statistical and scientifical data in the selection criteria of ELSE VP
2.3.1. The real number of SARS-CoV-2 infections >10 times more than the number of reported cases.
2.3.2. The importance of data and interpretations of the scientific literature.
2.4. Defining the selection criteria of the Vulnerable Patient
2.4.1. The significance of the comprehensive knowledge of the pathomechanism of the COVID-19
2.4.2. The preexisting conditions with COVID-19 caused severe diseases in accordance with CDC.
2.4.3. The percentages of death and preexisting conditions
2.4.4. Selected meta-analyses, systematic rewievs and other articles to help determine the selection criteria of Vulnerable Population
2.4.5. The significance of coexisting comorbidities to set up the selection criteria of VP.
2.5. Summarized parameters to finalize the selecton criteria of Vulnerable Population.
2.6. Defining the Number of ELSE VP
2.6.1. Defining the VP number from among chronic condition
2.6.2. Defining the VP number adapting the age stratified calculation of Imperial College
2.7. Isolating ELSE VP
2.7.1. Isolation of ELSE Vulnerable Population in Cruiser, Resorts and Hotels (VPCRH).
2.7.2. Isolation of ELSE Vulnerable Population in DISTRICTS (VPD)
2.7.3. Isolation of ELSE VP in Long Term Care Facilies.
2.7.4. Isolation of ELSE VP in Multigeneration population
2.7.5. Isolation of ELSE VP in villages
2.7.6. Scenarios
2.7.7. Necessary instructions for the ELSE Groups in order to avoid infection
2.8. Determining the Excess number of ICU beds for COVID-19
2.9. The High Effectivity of distinctive Non-Pharmaceutical Interventions (NPI) in ELSE
2.9.1. Classical and traditidional NPI and ELSE NPI
2.9.2. The Vulnerable Population (VP) Protocol for the VP members
2.9.3. The (EM)HQSB protocol for the whole ppl of the Age Groups (AG) (3.3 and 3.5.) Efficacy: 85%
3. RESULTS
3.0 Preliminary results and brief conclusion of the essence
3.1. Natural outbreak (NOB)
3.1.1. Natural outbreak without excess bed capacity
3.1.2. Natural outbreak with hypothetically unlimited number (25 000) of excess bed capacity
3.1.3. Natural outbreak with real (2 500) number of excess bed capacity
3.1.4. Natural outbreak with real number of excess bed capacity, with Season force intervention.
3.1.5. Natural outbreak with real number of excess bed capacity, for only two groups AG1 and AG2.
3.1.6. Comparison of the five Natural outbreak studies.
3.2. ELSE EM Epidemic model (EM) of ELSE 100% Efficacy
3.3. Epidemic model (EM) of ELSE, 85% Efficacy
3.4. VP protocol at 0th entry day for all AGs (AG1–4).
3.5. The system and efficacy of MIX VP-ELSE protocol
3.6. The influence of the gradually increasing (0-20-40-60%) level of the traditional NPI for the elderly group (AG4) in the combined MIX ELSE VP protocol.
3.7. The influence of the standard 60% NPI level for the two elderly groups (AG3, AG4) in the combination of MIX ELSE VP.
3.8. Final conclusion
3.8.1. Evaluation of the results.
3.8.2. Suggested phases of implementation of ELSE
4. DISCUSSION
4.1. The impact of COVID-19 on Socioeconomics and Health Care
4.2. Preventing the devastation effect of COVID-19 on socioeconomic by current NPI strategies.
4.3. Preventing the devastation effect of COVID-19 on socioeconomic by ELSE strategy.
4.4. The rationale behind the ELSE.
4.5. Opponents of the HI
4.6. Vaccine controversies
4.6.1. Vaccine global statistics
4.6.2. Vaccine statistics of Elderlies
4.6.3. Impaired function of vaccine in Elderlies
4.6.4. Rapid COVID-19 vaccine development and safeness
4.6.5. The development timeline of Vaccine
4.6.6. The transmission dynamics of superspreder events (SSE) and the preventing measures would substantivelyprolong the vaccine development
4.7. Importance of improving the innate immunity mechanisms against the COVID-19.
4.8. Ethical controversies.
4.9. The Importance of the Implementation
5. CONCLUSION
REMARKS
6. APPENDIX
6.1. Appendix 1
6.2. Appendix 2
6.3. Appendix 3
6.4. Appendix 4
6.5. Appendix 5
6.6. Appendix 6
6.7. Appendix 7
6.8. Appendix 8
6.9. Appendix 9
7. REFERENCES
The present study aims to contribute to the fight against coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), stating that the primary weapon of defense is the development of the most effective additional vaccines and antiviral drugs adapted to the mutants.
According to the unanimous opinions of the publications in prestigious papers, new waves caused by further SARS-CoV-2 mutants are expected. They can also develop from a genetic line other than Omicron and can cause serious illness for many years even if the pandemic turns to endemic.
SARS CoV-2 and its mutants will continue to target the life-threatening elderly Vulnerable Population (VP), especially those over 60 years of age who refuse vaccination, which accounts for only 0.1-0.3% of society. As a result, despite vaccination efforts to date, health care continues to be paralyzed due to the overcrowded intensive care units consequently causing severe losses in all areas of the economy and social life. In this context, the effectiveness of the current epidemic management practice could be significantly increased by introducing a special curfew of five days, limited only to the time of peaking of recurrent epidemic waves, in accordance with 1.15.3. as described at the end of this chapter.
The future solution to further waves or even endemic conditions could be a new-minded strategy to place sick refusers over the age of 60 in some specially prepared “COVID specialist hospitals” in the vicinity of major county hospitals. The functions of these small hospitals will be temporarily taken over by those nearby county hospitals.
In addition to the above priority, it is necessary to simultaneously introduce a curfew for those who refuse to be vaccinated over the age of 60 and to offer physical protection, the common result of which is equivalent to compulsory vaccination, but in this way the protest against compulsory vaccination can be prevented.
The role of innate immunity is absolutely crucial for children, where the author draw a detailed attention for considerations of the vaccination. In particular, vaccination of healthy children under 12 years of age has recently been suspended (!) In the United Kingdom and Sweden, according to comprehensive, convincing researches. It is becoming increasingly clear that “innate immunity balance” is the decisive factor for all ages and explains the development of COVID-19, including the “cytokine storm”.
As a typical member of the Vulnerable Population, after three vaccinations, the author states that the primary weapon of defense is the targeted, effective vaccination.
Suspension of vaccination in children is justified for several reasons:
- Firstly, the possible negative effects (ADE, Autoimmune cases, etc.) of current and emerging vaccines cannot be ruled out. Based on current scientific findings, there is a chance that such adverse events will occur.
- Secondly, the survival rate (CDC) among young people is 99.998%, with two out of a million dead, half of whom have MIS-C (multi-system inflammatory syndrome in children). In their case, rare severe diseases have been shown to have a predominantly genetic background that generates a predisposition state. They are also part of the VP and vaccination is recommended for them. The majority of them survive the infection asymptomatically or with mild symptoms and have been shown to be more effective through natural infection through antibodies against multiple viral epitopes and cellular immunity that have been shown to be more effective than vaccines that produce the same one type of antibody. In addition, vaccinations administered to the upper arm muscle bypass the innate and superficial mucosal IgA immune defense system that is activated by the natural route of infection, which in their case alone can be sufficient to combat COVID-19.
- Thirdly, the fact that the increasingly threatening new mutants, which have higher transmission dynamics (R0 = 6) and the ability to break through individual immunity developed by the previous variants and / or vaccines, the required level of necessary herd immunity (HI) to provide protection for all has been raised to 90%. This level cannot be achieved by vaccination alone, only as a combined result of vaccinations and natural infections by those who have not been vaccinated.
- Finally, the suspension of vaccines in children may be justified alone by the fact that vaccines do not prevent the spread of delta mutants.
As detailed in the Introduction, vaccinating healthy children serves no purpose other than to protect the elderly at-risk Population, who make up only 0.1-0.2% of society. Moreover, it cannot really serve this purpose either, as vaccinating children does not have a particular effect on the transmission they exert.
Despite the surge in mass vaccinations, the next waves of new mutants will cause deaths to jump again and restrictions may need to be re-introduced, reluctantly or not at all willing to submit to the hardest hit working age groups (restaurants, events, etc.). This civil resistance will further pave the way for a much freer and more destructive spread of SARS-CoV-2. The situation may become even more unpredictable due to the decreased immune response of the elderly to vaccinations.
A unique feature of SARS-CoV-2 is that the virus threatens only one personally identifiable narrow Vulnerable Population with severe or fatal consequences, predominantly the elderly which are suffering from various chronic conditions (2.5). This is still true with the unfortunate proliferation of new mutants, where several younger victims are present, but more than 90% of the victims are still characteristic from the aforementioned VPs over the age of 60.
Based on the CDC evidence lists (2.4.2), the study summarizes all relevant meta analyzes, systematic reviews, and statistics in the literature to determine age and other health parameters (2.4.4) and associated diseases (2.4.5.) the expected severity and outcome of COVID-19 should be estimated. Based on the guidelines and scoring system set up in this way (2.5), the scoring system is finalized individually by the local health authorities and in particular, by GPs who know them personally with their illness.
Campaigners against extreme vaccination are to be condemned. However, the judgment of insecure ordinary people is greatly affected by the current communication turmoil, so it is our moral duty to protect them as well. If we cannot offer them safe livable physical protection through isolation, it is questionable whether health and socio-economic life can resume due to ongoing deaths. If, on the other hand, we provide them with this isolation, the issue of civil liability will come to the fore and they can only blame themselves for the consequences. From now on, society has no obligation to give priority in the health care system to those who deny the possibility of both biological (vaccination) and physical protection (isolation).
These proposals for measures offer a morally and ethically unquestionable solution to the fight against the pandemic, as we also have a responsibility to create a normal life for the working age group of the remaining 99% of society and to prevent future irreparable injuries to younger age groups from permanent school closures. Society has suffered more than $ 10 trillion in losses worldwide so far and made incredible efforts to reduce the deaths of less than one percent of people, resulting in multiple direct and indirect deaths in the other 99%, mostly working age, as a result of QALY, WELLBY and other calculations.
Preventive intensive care alone costs for example more than physical protection (2.7.1) and the current state subsidy for empty hotel beds is significant. And the lives saved cannot be expressed in numbers.
The procedure would be essentially voluntary. Plenty of high-quality reception capacity is available and not only for 0.1–0.2% of unvaccinated vulnerable people, (2.7) but also for Hungary, for example, up to 2% of the population can command and manage defense work
The efficacy of vaccines may be largely offset by the higher transmission dynamics of new mutants, their ability to reinfect, their ability to bypass the immune response, the reduced immune response of the VP, and the civil resistance to further limitations.
The reasoning in the book is justified by time and events. The examples of China and North Korea make it clear that the key to effective and efficient epidemic management is not a continuous escape from the virus, but a new approach to targeted preparedness and strong measures focusing on the most affected populations. It is not necessary for society as a whole to endure from time to time the drastic hardships that result from closures that delay only the solution of a problem. On the other hand, in addition to, of course, vaccination at the highest possible population level, it is sufficient to prescribe moderate measures (use of a mask) for the active working population during the epidemic peaks. At the same time, however, it is necessary to make the "COVID specialist hospitals" ready and to take the above-mentioned measures against those who refuse to be vaccinated over the age of 60.
ELSE can supplement the level of herd immunity developed by 60-80% vaccination in the developed world to achieve population-level protection while minimizing deaths, which is important for the developing regions where vaccination is only 5%. By using of ELSE and COVAX together, herd immunity can quickly catch up with the developed world, and if they can reach at a protective level on all continents at the same time, there is a chance of eradicating the virus globally.
| ACE2 | angiotensin-converting enzyme 2 |
| ADCC | antibody dependent cellular cytotoxicity |
| ADE | antibody-dependent disease enhancement |
| BALT | bronchus-associated lymphoid tissue |
| BMPC | bone marrow plasma cell |
| AG | age group |
| CD | cluster of differentiation |
| CDC | Centers for Disease Control and Prevention |
| CI | case isolation |
| COVAX | COVID-19 Vaccines Global Access |
| COVID–19 | coronavirus disease 2019 |
| CP | Control Panel |
| DALY | Disability-adjusted Life Year = YLD+YL |
| ECD | European Control Desease |
| ECMO | Extra Corporal Membrane Oxidation |
| FDA | Food and Drug Administration |
| GUI | graphical user interface |
| GVH | Graft Versus Host |
| HCoV | Human Coronavirus |
| HCT | Human Challenge Model |
| HI | Herd Immunity |
| HLA | Human Leukocyte Antigen |
| HQ | Home Quarantee |
| ICI | Immun Checkpoint Inhibitor |
| ICU | Intensive Care Unit |
| ID | immundeficiencia |
| IFN | interferon |
| Ig | immunglobulin |
| IHME | Institute for Health Metrics and Evaluation |
| ILC | Innate Lymphoid Cell |
| Imp. Coll. | Imperial College |
| IL | interleukin |
| JAMA | Journal of American Medical Association |
| JCVI | The Joint Committee on Vaccination and Immunisation |
| KIR | Killer Immunoglobulin-like Receptor |
| LLPC | long-lived plasma cell |
| LSTH | London School Trophical and Higiene |
| LTCF | Long Term Care Facilities |
| MAIT | mucosa-associated invariant T cells |
| MALT | mucosa associated lymphoid tissue |
| MHC | Major Histocompatibility Complex. In human beings the complex is also called the human leukocyte antigen (HLA) system. |
| MIS-C | Multisystem Inflammatory Syndrome in children |
| NALT | nasopharyngeal-associated lymphoid tissue |
| NEJM | New England Journal of Medicine |
| NET | neutrophil extracellular trap |
| NHS | National Health Service |
| NOB | Natural OutBreak |
| NPI | Non Pharmaceutical Interventions |
| ORF | open reading frame |
| PC | public closure |
| PPL | population |
| QALY | Quality Adjusted Life Year |
| RBD | receptor-binding domain |
| S - S1 | spike protein - spike protein one subunit |
| SAGE | Scientific Advisery Group for Emergencies |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| SDO | Social Distance Oldies |
| SEIR | Susceptible Exposed Infectious Recovered |
| sIgA | secretory IgA |
| Tc | cytotoxic T cell |
| TESSy | The European Surveillance System |
| Tfh | follicular helper T cells |
| TLR | Toll-like receptor |
| TNFα | tumour necrosis factor alpha |
| TRM | tissue resident memory T-cells |
| UCLA | University of California Los Angeles |
| VP | Vulnerable Population |
| VPCRH | Vulnerable Population Cruises Resorts Hotels |
| VPD | Vulnerable Population District |
| WELLBY | Well-Being-Year |
| YLD | Years Lived with Disability |
| YLL | Years of Life Lost |
As the scope of the book is far beyond its usual publications, the explanation of certain key abbreviations is sometimes repeated for different fluency (contrary to the requirements of the publications) (eg VP - Endangered Population).
By clicking on “back to the table of contents” at the end of each chapter, the cursor will jump back to the Table of Contents, where clicking on any chapter again will make the chapter you are looking for immediately visible. Similarly, for links or references clicking will jump to the specific link or reference within the list of links at the end of the book (References), and then click again to return to the original context.
For pulications, click on the DOI ID (e.g. doi: https://doi.org/10.1038/d41586-022-00215-2) , or the normally underlined blue link (https://media.nature.com/lw800 /magazine-assets/d41586-020-02544-6/d41586-020-02544-6_18347822.gif) and the underlying content is displayed on the reader screen.
{kind=link}
In the English version of the book, the identifier of the study is the acronym “ELSE,” which stands for Elderly Life Saving Emergency. The sentences or phrases where the word ELSE occurs should be interpreted as the title of the study accordingly. The fight against COVID-19 is important “before everything ELSE”.
Once again: According to the unanimous opinions of the publications in prestigious papers, new waves caused by further SARS-CoV-2 mutants are expected. They can also develop from a genetic line other than Omicron and can cause serious illness for many years even if the pandemic turns to endemic.
The word “endemic” is coupled with false promises in lay public opinion that COVID-19 is, so to speak, “decaying” naturally, and evolution somehow taming the pathogen so life simply returns to normal.
However, there is no pre-determined evolutionary program to make a virus more benign, especially those such as SARS-CoV-2, in which most infections occur days before the onset of symptoms or the onset of a serious illness. Not to mention that Alpha and Delta have become more virulent than the tribe first found in Wuhan, China.
During endemic infection, the overall transmission rate is static. The infectivity rate equals the viral reproductive baseline (R0), the number of individuals that an infected individual would infect, assuming a population in which everyone can become ill (e.g., common cold, fever, malaria, etc. are considered endemic).
However, an endemic disease can spread to a wide population, infecting a large number of people and being fatal. Malaria caused more than 600,000 deaths in 2020. Ten million became ill with tuberculosis in the same year and 1.5 million of those died.
In light of the above, we examine the questionable optimism generated by Omicron regarding the end of the epidemic and the expected future outlook for COVID-19 (maybe from now on 23-24-25…, etc.). Among the mutant variants so far, a couple could have earned another year…
For that purpose, let us look at the relevant - and unfortunately, consensual - opinions of prominent researchers who have been working on the subject from the beginning of the outbreak in articles in this year's issues of Nature. Subsequently, the views of scientists in the Nature articles are confirmed by a report published by the UK Scientific Advisory Board (SAGE) with a deep scientific basis.
Scientists are constantly examining three theories. One is the mutation that was not found. Although researchers have sequenced millions of SARS-CoV-2 genomes, they may have simply omitted a series of mutations that eventually led to Omicron. Alternatively, the variant may have developed mutations in a person as part of a long-term infection. Or it may have appeared invisibly in other animal hosts such as mice or rats.
The first article deals with the origins of Omicron: {*}
Scientists are constantly examining three theories. One is the mutation that was not found. Although researchers have sequenced millions of SARS-CoV-2 genomes, they may have simply omitted a series of mutations that eventually led to Omicron. Alternatively, the variant may have developed mutations in a person as part of a long-term infection. Or it may have appeared invisibly in other animal hosts such as mice or rats.

Figure 1.1. shows that the Omicron is so different from previous variants that evolutionary virology scientists estimate the presence of the earliest genetic predecessors more than a year ago. (Taken from reference 1)
“It simply came out of nowhere” (Darren Martin, University of Cape Town in South Africa).
“However, SARS-CoV-2 has not yet explored its full potential in humans. The virus is still spreading in the evolutionary trajectory. Indeed, Omicron shows that we need humility to think that we are able to understand the processes that are shaping the evolution of viruses like SARS-CoV-2 ”(Jesse Bloom, Fred Hutchinson Cancer Center, Seattle
In the second, experts comment on whether Omicron could end the pandemic: {*}
Although the rapid spread of Omicron, the different vaccine strategies, and the changing immunity around the world make it difficult to model the future of the pandemic, scientists are unanimous that Omicron is far from over and in a very long time, even decades, could it evolute and/or transmute into a balanced endemic.
“While vaccines are likely to continue to provide protection against severe symptoms, Pagel says the infection will continue to spread. There is a growing perception that none of the vaccines provide long-term protection against infections” (Christina Pagel, University College London). "I don't think vaccinations are the way out of this pandemic." (Julian Tang, Leicester Royal Infirmary UK)
„COVID-19 will truly become endemic only when most adults are protected against severe infection because they have been exposed multiple times to the virus as children, and so have developed natural immunity. That will take decades, and it means many older people today (who were not exposed as children) will remain vulnerable and might need continued vaccinations.” (Mark Woolhouse, Government Adviser, University of Edinburgh, UK)
It won't end with Omicron, the researchers predict. “It won’t be the last version, so the next version will also have its own specialty. Given that there is no chance that the virus will disappear completely, COVID-19 will inevitably become endemic over time. ” (Graham Medley and Sebastian Funk are government advisers to the London School of Hygiene & Tropical Medicine).”There is no guarantee that the next version will be lighter." declares Julien Tang.
The topic of the third article is the unavoidable a new mutant variants: {*}
Scientists say the emergence of the new mutated variant is only a matter of time.
“I think it’s inevitable to see new variants with varying degrees of immune avoidance. There is no guarantee that the next dominant version will sprout from the “mild” Omicron branch of the SARS-CoV-2 family tree. It is possible that a later version may revert to the descendant of Delta or Alpha, with sufficient immune avoidance to sweep Omicron. They can come from anywhere, especially where the virus is widespread”(Andrew Rambaut, University of Edinburgh UK).
"The next mutated variant may have other properties. I don't think there is any guarantee that these properties will be worse, as such viruses are unpredictable. This fills me with a bit of fear" (Wendy Burgers, University of Cape Town in South Africa)
Closely related to and systematized above, the UK Scientific AdvisoryBoard (SAGE) has raised, inter alia, the possibility that SARS-CoV-2 may become more severe or prevent current vaccinations by recombination with other coronaviruses. Continuous circulation in animal reservoirs offers several possibilities for surprising changes such as bypassing immune defense or increased severity. The following is an abbreviated topic of this SARS-CoV-2 research and analysis (Long Term Evolution of SARS-CoV-2 July 2021): {*}
„Can we predict the limits of SARS-CoV-2 variants and their phenotypic consequences?
As eradication of SARS-CoV-2 will be unlikely, we have high confidence in stating that there will always be variants.
We describe hypothetical scenarios by which SARS-CoV-2 could further evolve and acquire, through mutation, phenotypes of concern, which we assess according to possibility. For this purpose, we consider mutations in the ‘body’ of the virus (the viral genes that are expressed in infected cells and control replication and cell response), that might affect virus fitness and disease severity, separately from mutations in the spike glycoprotein that might affect virus transmission and antibody escape.
We assess which scenarios are the most likely and what impact they might have and consider how these scenarios might be mitigated. We provide supporting information based on the evolution of SARS-CoV-2, human and animal coronaviruses as well as drawing parallels with other viruses.
Scenario 1: A variant that causes severe disease in a greater proportion of the population than has occurred to date
For example, with similar morbidity or mortality to other zoonotic coronaviruses such as SARS-CoV (~10% case fatality) or MERS-CoV (~35% case fatality).
This could be caused by:
1. Point mutations or recombination with other host or viral genes…”
„2. By recombination between 2 VOC or VUIs…”
Likelihood of genotypic change in internal genes:
Likely whilst the circulation of SARS-CoV-2 is high.
Likelihood of increased severity phenotype:
Realistic possibility.
Impact:
High…”
“Scenario 2: A variant that evades current vaccines
This could be caused by:
Antigenic ‘shift’
3. Natural recombination events that insert a different spike gene sequence (or partial sequence) from human CoVs MERS-CoV (highly unlikely due to the low frequency of MERS-CoV infections), or from currently circulating endemic human CoVs (more likely due to the prevalence of these viruses). This would recombine into the ‘body’ of SARS-CoV-2 that is capable of high replication in human cells. The consequence could be a virus that causes disease at a level similar to COVID-19 when it first emerged but against which our current battery of spike glycoprotein-based vaccines would not work.
Likelihood:
Realistic possibility.
Impact:
High for a completely new spike, medium or low if a spike from a seasonal CoV is introduced since we expect a proportion of the population to have antibodies to these endemic viruses…”
„Longer-term shift
4. A longer-term version of shift whereby SARS-CoV-2 undergoes a reverse zoonotic event into an animal reservoir(s). This virus is then on a separate evolutionary trajectory because the virus animals is subject to different selection processes than in humans. The SARS-CoV-2 decedents then re-emerge into humans at a later time when vaccines that have been updated to keep pace with drift in humans sufficiently mismatched so as not able to provide immunologic cross protection.
Likelihood:
Realistic possibility.
Impact:
Medium…”
„Antigenic drift
5. A gradual or punctuated accumulation of antigenic variation that eventually leads to current vaccine failure. Worst case is that this drift combines with significant antigenic sin (vaccination resulting in an immune response that is dominated by antibodies to previously experienced viruses or vaccines) meaning that it becomes difficult to revaccinate to induce antibodies to the new strains. Genetic and antigenic drift are almost inevitable. Antigenic sin has not yet been reported for SARS-CoV-2 so we consider this possibility less likely.
Likelihood:
Almost certain.
Impact:
Medium...”
„Scenario 3: Emergence of a drug resistant variant after anti-viral strategies
This could be caused by:
6. Emergence of new variants following the administration of directly acting antiviral therapies. As we begin to use directly acting antiviral drugs it is highly likely a variant will be selected that had resistance to individual agents. For example, drugs that target the viral 3C protease, drugs that target the polymerase, monoclonal antibodies that target the spike glycoprotein. If the drugs are used as a mono therapy, then resistant variants have a high probability of emerging. This may render all drugs in that category unusable.
Likelihood:
Likely - unless the drugs are used correctly.
Impact:
Medium unless a scenario arises where drugs are needed more widely...”
„Scenario 4: SARS-CoV-2 follows an evolutionary trajectory with decreased virulence
This could be caused by:
7. Variants arising with increased transmissibility but decreased pathogenesis or virulence as the virus becomes fully adapted to the human host becoming an endemic infection. Coupled with the likelihood of eventual high populations immunity the infection produces less disease. In other words, this virus will become like other human CoV that causes common colds, but with much less severe disease predominantly in the old or clinically vulnerable.
Likelihood:
Unlikely in the short term, realistic possibility in the long term...”
It is clear from the above that current cyclical restrictive measures (social distance) are hampering the evolutionary trajectory of the virus. These delay the development of an endemic “resting state” as soon as possible with less severe cases. On the other hand, by exerting a constant selection pressure over time, especially including the effect of the new vaccines (1.7.3.) they predispose to the development of newer and newer mutations that are getting worse and more unpredictable.
The present study (ELSE) also helps to address this, as it eliminates the need for current cyclical restrictive measures in addition to reducing deaths and facilitates the development of an endemic – hopefully - “rest state” as soon as possible.
Protecting health and well-being means that balancing the health risks and health, social and economic costs of COVID-19 is paramount. ELSE effectively reduces all of these risks and costs. Current control strategies are based on the repetitive implementation of restrictive measures, testing and related contact discovery. The essence of this suppression - mitigation strategy is the cyclical application of austerity measures to prevent overloading the health care system. {*}This process can take up to several years (more than two years so far) and up to 10 interventions (five are over) until natural and vaccinated herd immunity develops.
The more successful the restrictive measures, the more intense the next wave can be expected. Without a plan to eradicate the virus, countries could face downtime over and over again, scientists warn, and the protracted strategy will produce increasingly aggressive mutants that will push the population-level herd immune threshold to the unattainable 90% with emerging vaccine resistance. {*}
Understanding the dynamic evolution of herd immunity through restrictive measures and vaccination is important to protect the population. {*} The virus is more likely to infect those who do not vaccinate themselves due to the expected higher herd immunity, leading to a higher mortality rate among its at-risk population members (0.1-0.2% of the total population).
Consequently, the importance of a successful global collaboration (e.g. the combination of the ELSE and COVAX and the further development of them into an international “master plan”) is particularly important because otherwise the virus is likely to remain between us for an unpredictable period of time. In connection with this, the strategy of ELSE is extremely important, because this new approach, including the isolation of the Vulnerable Population, enables the normal functioning of socio-economic life and the health care system with a minimal number of deaths.The interaction between SARS-CoV-2 and the Endangered Population (VP) results in the intermittent absence of intensive care beds and ventilators at the peaks of recurrent epidemic waves. Therefore, coronavirus 19 infection (COVID-19) is considered to be an emergency of less than 1% of identifiable, physically separable VPs in the elderly, which periodically represents an unprecedented crisis for public health and, consequently, for social life and the economy globally. If the intensive care units were not saturated beyond the peak of the epidemic waves, neither the hospitals nor the economy would be paralyzed. Thus, for example, there is no limit to the timing of influenza pandemics because neither the intensive care units nor the economy are paralyzed. However, there are 6 deaths per million young people under the age of 18 vaccinated against influenza, while only 2 out of one million young people under the age of 18 unvaccinated against COVID-19, {*} who, in contrast to influenza cases, suffer from well-identifiable comorbidities and of course, should be vaccinated. {*} (For an analysis, see Introduction Chapter 1). According to a shocking publication in the latest CDC study published in this year's JAMA, the risk of myocarditis has increased in all younger age groups after mRNA-based injections, but with particularly severe consequences after the second (!) vaccination among adolescents. {*}
SARS CoV-2 and its mutants attack in a life-threatening manner only those elderly Vulnerable Population (VP), who refuse vaccination and make up only 0.1-0.3% of the society, in a way that
- hospitals are overwhelmed by waves and are overburdening other departments,
- who paralyze the health care system and, consequently, the economy, everyday life,
- which may be exacerbated in the long run by school closures and planned vaccination programs for children, which call for greater thought.
In the current situation, the most effective way to combat COVID-19 is to use the following measures and solutions or a combination of them. These apply to those over 60 years of age who refuse to be vaccinated, who account for more than 90% of expected serious or fatal cases.
As a matter of priority, the introduction of care in specially designated and professionally prepared “COVID special hospitals” for those over 60 years of age who become infected or become ill should be recommended.
Currently, at the time of the epidemic, virtually all intensive care units in the country are involved in the care of COVID-19 patients. If a ventilator is required, this means, in practice, admission to an intensive care unit, which means the full commitment of the expanded equipment for other cases, which is not necessarily required for the supply of COVID-19, and the correspondingly highly trained staff. Of course, extremely serious cases - where, for example, there are already signs of multiple organ involvement - are an exception. "COVID specialist hospitals" could prevent national congestion by:
- Depending on the intensity of the epidemic and the need, in due time and intermittency, the usual responsibilities of some of the small hospitals designated for this special hospital function will be taken over by the nearby major county hospitals.
- At the same time, the already selected, specially trained and even multi-paid staff from the regions will take over from the vacant patient rooms of small hospitals between the professional standards of the ward and the intensive care unit.
- The intensive care team of small hospitals will remain on site as the professional supervisor and coordinator of COVID-19 patient care. In this way, patients can be grouped with sufficient flexibility within the three wards of the existing intensive care, sub-intensive and non-serious hospitals.
That measure is professionally and epidemiologically justified. It is difficult to find a counter-argument against it.
This strategy is also justified by:
- The vast majority of serious and fatal cases of COVID-19 are those who refuse vaccination over the age of 60, who occupy the intensive care and other important wards of county hospitals at the national level and burden them for a long time and their professional staff.
- The combination of these unresolved urgent and non-urgent cases and other negative socio-economic consequences, according to DALY, WELLBY, QALY calculations, causes more than ten times as many deaths among young people.
- As a result, the national workload falls to a fraction, allowing normal health care to continue, making crippling restrictions, school closures, etc. unnecessary.
- “COVID specialist hospitals” can provide more efficient, massive and concentrated care that can provide a buffer of adequate magnitude in the event of a wave of any intensity so that standard patient care at the national level can continue in the usual channel. In addition, through appropriate segregation of duties, they increase systemic health gains, enabling society and the economy to lead a normal life.
In addition to the strategy based on 'COVID specialist hospitals', it is necessary to introduce a severely sanctioned curfew for those who refuse to be vaccinated over the age of 60 and, alternatively, to offer physical protection equivalent to vaccination.
- Introduce a severely sanctioned curfew for those who refuse to be vaccinated over the age of 60 for the duration of the wave(s). Of course with the community solution of everyday care (see 2.7.7.).
- Offering physical protection equivalent to vaccination for those who refuse vaccination over the age of 60. This separation would take place in safe, cultured, livable conditions, which is detailed in the study. The ELSE study demonstrates that with careful professionalism and discipline, it is indeed possible to safely isolate this Vulnerable Population during the period of recurrent waves until a sufficiently effective vaccine, even for them against mutants is developed. The technical side of designing and implementing secure isolation requires guidance and direction by military logistics experts. (4.9.).
With the exception of a fraction of a percent of the elderly, the measures above allow all of the society the followings:
- Society is no longer obliged to give priority in the health care system to those who reject both biological (vaccination) and including the measures to be taken, the possibility of physical protection (isolation).
- Society also has a responsibility to others, - to put it bluntly, as more than 99% of fellow citizens affected by incarceration already represent themselves, whose loss of quality of life and short- and long-term quality of life due to incarceration is a scientifically developed and accepted measure, based on more than ten times the sacrifice equivalent of offering.
- This morally justifiable new social attitude can make a significant contribution to curbing anti-vaccination behavior, especially for the population, which is even more at risk of their lives.
- This way, overcrowding in intensive care units can be prevented and deaths can also be almost completely prevented.
- The normal operation of the health care system and socio-economic life can be ensured even in the event of the next wave (s), as restrictions and school closures become unnecessary.
On the other hand, it is of paramount importance that among those who refuse vaccination over the age of 60, the measures mentioned above and / or the physical protection offered provide an opportunity to suspend vaccination for younger generations, especially under the age of 12, for a number of reasons:
Less than 2% of young children under the age of 18 were diagnosed with COVID-19 infection{*}, most of which were mild or asymptomatic{*}. Researchers at Imperial College and other excellent British universities say that COVID-19 infection in children and adolescents requires extremely rare intensive care (PICU) and very few deaths in the first year after the pandemic broke out. Of the population of children and juveniles in the UK, there were 2 deaths out of 1 million, half of whom already had a fatal illness. Admitted to the PICU from the pediatric and juvenile population, in addition to the pre-existing severe disease, they were more likely to be older and more colorful.{*} {*} {*}
In general, children and older adults are the most sensitive to other viral infections, and the risk of severe infection can be described by a U-shaped equation / curve. In the case of COVID-19 infection, there is no increase in the number of cases in young people, the curve only curves upwards in the elderly.
The low risk of complication of COVID-19 infections in children and adolescents can be well illustrated by comparing them with influenza virus infections. In the United States, the influenza virus vaccination rate in that population is 50.4%. There were 434 deaths in the 0-17 age group of 70 million, representing 6.2 deaths per 1 million children and adolescents with a 50% vaccination rate.{*} 2 deaths per million people with COVID-19 infections at 50% vaccination could theoretically mean 1 person per 1 million people, so at the same level of transmission of influenza virus and SARS-CoV-2, we would expect 6 times the number of deaths from influenza virus.
COVID-19 infection in children (including infants under 1 year of age) does not cause more severe symptoms than other human coronavirus or influenza virus infections. Based on studies led by Vanhems P and Yilmaz K, time to hospitalization, need for intensive care and respiratory support, and mortality were proportionally higher in patients with rhinitis (i.e., influenza and human coronavirus infection) than in COVID-19-infected individuals.{*} {*}
A comparison from the CDC database in September 2021 leads to a similar conclusion.{*}
According to a study from Kings College, only 1.8% of adolescents had post-COVID-19 syndrome that lasted longer than 56 days. Common symptoms were fatigue, headache, and loss of smell. In only 4.4% of children infected with symptomatic COVID-19, acute infectious symptoms persisted for more than 4 weeks, in which case the intensity of symptoms continued to decrease. In almost all children the infectious symptoms ceased within 8 weeks.{*} The data above also suggest that post-COVID-19 syndrome is very rare in children.{*}
Also, data from Kings College and University College London (UCL) show that the symptoms of Delta variant infections do not differ significantly from the Alpha variant in school-age children, either in the type of symptoms or in the duration of infection. Infectious symptoms largely resolved within 28 days. The significance of the studies above is that they also provide a large amount of data for cases of infection caused by the Delta variant in deciding whether children should be vaccinated.{*}
Overall, among healthy children and adolescents, the number of clinically severe infections, post-COVID-19 syndrome, and deaths is negligible compared to other respiratory viruses, from influenza to RSV (Respiratory sycitial virus) infection.
Identifying children and adolescents at risk of severe SARS-CoV-2 infection is important in establishing a vaccination strategy{*} Vaccination of healthy children aged 12-15 years has been suspended in Sweden and the United Kingdom following the selection of children at risk.
In the United Kingdom, the Joint Committee on Vaccination and Immunization (JCVI) concluded on 31 August 2021 that “the minimum health benefit of vaccinating children is not equivalent to the potential health damage caused by it, as the level of uncertainty is too high, regarding the number of potential harms / injuries. As the health benefits of vaccination are currently too small, it is not advisable to recommend vaccination of otherwise healthy children aged 12-15 years”. In the JCVI statement the comorbidities are listed when the children are recommended to be vaccinated.{*}
In Sweden, similarly only those aged 12-15 who suffer from some form of lung disease, asthma, or some high-risk comorbidity are vaccinated. {*}
The Swedish government largely lifted restrictions on COVID-19 infection on 29 September 2021 due to high vaccination rates, but also took into account the burden on health, mortality rates and the risk of increased transmission of the infection.{*}
Based on the above provisions and the clear recommendations of these two European countries and recently California{*} 27 only vulnerable populations should be vaccinated in children and adolescents.
The above view is supported by an early study from overseas Univerity of California that suggests a vaccination policy for 12-15 and 16-17 year olds, as the risk of developing post-vaccination myocarditis is higher than a hospitalization caused by possible COVID-19 infection{*}
Children are not the primary vectors of the virus and the extent of possible transmission is independent of whether they are vaccinated or not.
WHO statements of 22 September 2021:
1) "Most children have a low risk of developing a serious infection, so vaccination is given primarily to reduce transmission"
The statement raises moral issues, as children are not vaccinated to protect themselves from the disease, as this is not the only way they should be vaccinated, but primarily to protect others (who are unwilling to vaccinate themselves) by (presumably not proven) to spread fewer viruses.
2) "COVID-19 vaccines are effective in preventing the development of serious infections and reducing fatalities, but infection and reinfection are possible after vaccination."{*}
Thus, according to the statement, children are vaccinated in vain, yet they can become infected again and remain infected.
So the only rationale for the argument is that if children are vaccinated, perhaps fewer of the virus they spread and a similarly well-founded estimate of about 10 million innocently vaccinated children will prevent the death of 1 elderly individual in a VP who refuses to be vaccinated.
This further strains the moral issues already mentioned along biomedical ethical principles: To what extent do we i) respect the autonomy of children, ii) not harm them, iii) benefit the intervention, and finally iv) how fair are they?{*}
This contradicts the findings of Dr. Kathrine O’Brien, a member of the WHO Commission, on vaccination:
"… First, the main function of the vaccine is to protect the recipient against infection…"
"… Secondly, in the event of an infection, it reduces its severity…"
"… Third, to reduce the transmission of the virus"{*}
The logical consequence, according to Dr. Kathrine O’Brien’s findings - which contradicts the WHO’s September 22, 2021 statement - is that if children did not spread the virus, they would not have to be vaccinated. In school children, the rate of SARS-CoV-2 infection is low, the possible infection is mild or asymptomatic, and transmission of the virus is uncommon.
It has been observed that the spread of the infection is more between different generations than siblings passing the virus to each other, an observation that could help organize measures for public schools, parishes and kindergartens later in the pandemic.{*}
Vaccination of children and adolescents is of questionable significance for viral transmission between each other and directly to the larger population inoculated from them. Estimates differ significantly, with “JCVI committe” suggesting a small effect on young vaccination, as vaccinatio did not play a major role in the transmission of the Delta variant.{*}
A “Nature” article highlights the statements of a UCL scientist that “the physical (school closure) and biological (vaccination) protection of children may have done more harm than good”. Imperial College London scientist Elizabeth Whittaker says “Shields are very leaky”, “measures to provide physical and biological protection are not perfect and are likely to have caused more stress and anxiety to families than benefits”{*}
The opening of schools has had minimal consequences for the overall transmission of SARS-CoV-2 virus to the population.{*} So the school closures have no effect on transmission. In Sweden, public education for 6-16 year olds did not stop during the pandemic, school closures were not considered an appropriate measure, citing the potential harm and consequences of school closures to society as a whole. {*}In summary:
It is true that the spread of SARS-CoV-2 occurs in schools, but this is not significant for all cases of COVID-19 infection.
If appropriate measures are put in place in schools, schools will not play a significant role in the transmission of the virus.
From the point of view of cost-effectiveness, as schools are an essential part of the functioning of our society and the lives of children, their closure is unnecessary, if the introduction of other measures to prevent the spread of the virus proves ineffective.
What is the point of further reducing transmission? To protect those elderly VPs who refuse to take the vaccine? It is a completely incomprehensible solution with unforeseeable consequences, with huge sacrifices and costs, with a common social insight. Everything for nothing?
The second question in our study is: Based on the above data and studies, what is the rationality behind school closure?Most studies of COVID-19 infection focus on the white blood cells, serum immunoglobulins, and systemic cellular immune response of the immune system. However, most immune cells, including 95% of T cells, are found and function in tissues, mostly in lymphatic organs such as bone marrow, spleen, lymph nodes, and on protective membranes, surfaces such as skin, intestines, and mucous membranes of the upper (nasopharynx) and lower protective respiratory tract (bronchi, alveoli).
SARS-CoV-2 first infects the epithelial cells of the upper respiratory tract. The early immune response in the mucosa begins with antigen priming, a dynamic, localization-assisted compartmentalized defense network based on the interaction of the innate and adaptive immune systems. Its initial site of induction is in the nasopharyngeal-associated lymphoid tissue (NALT), and later the infection elicits an immune response from distant sites, including the tracheobronchial epithelium, the regional lymph nodes. NALT is part of the mucosa associated lymphoid tissue (MALT), one of its anatomical compartments.
In addition to NALT, the pharynx and tonsils are a special representation of MALT{*}, consisting mainly of B cells (65%), CD3 + T cells (30%), of which 80% are CD4 + T cells and macrophages (5%).{*}
According to research by Mount Sinai scientists, the expression of the ACE2 gene on nasal epithelial cells varies with age, according to which it is less frequent in children than in adults (ACE2 receptor expression is minimal at age 10, then begins to increase). Because the virus enters the cell through the ACE2 receptor, a lower dose of the virus is found in children after exposure to the same virus. This may also explain why COVID-19 is more common in adults.{*}
Furthermore, according to research by Albert Einstein Coll. Med., Early mucosal immune responses in children are much more intense than in adults. The mucous membranes lining the airways have a higher duration of interferon-γ and interleukin-17 signaling proteins in children, {*} which alert the immune system to incoming pathogens and contribute to the activation of the innate (or non-specific) immune system, which plays a greater role in eliminating the virus in children compared to the immune system.{*}
In the respiratory tract, a robust non-specific immune response, the early IgA burst, rapidly and efficiently eliminates the virus, leading to a complete failure of the specific immune response in the defense, leading to the development of a mild or asymptomatic COVID-19 infection clinically.{*}
The Francis Crick Institute has been investigating the cross-reactivity of antibodies to human coronavirus (HCoV) infections that cause seasonal rhinitis and thus humoral immunoprotection in COVID-19 infections. As HCoV is most prevalent in children, it is not surprising that it was highest in the 6–16-year-old age group: 62% IgG cross-reactivity, where HCoV seroconversion was highest, and this cross-reaction was significantly higher than in adults. {*}
Based on the epidemiological experience of a large cohort study, SARS-CoV-2-infected individuals who had serologically confirmed HCoV infection in the previous 3 years had a lower risk of severe COVID-19 infection, leading to intensive care unit care. {*}
The third question in our study is: What is the rationality of vaccinating children if it is designed to bypass the important upper respiratory mucosal immune system?
Natural killer cells play a crucial role in maintaining immune homeostasis, on the one hand through the non-specific immune system, where it provides first-line protection against pathogens and cancer cells, and on the other hand, by contributing the activation the specific, adaptive immune system.
All healthy cells with a nucleus in the body express the major histocompatibility complex I (MHC I) on the cell surface, indicating to NK cells that it is an “own” cell belonging to the organism. MHC I complex binds to the NK cell as an inhibitory ligand, thereby tolerating and not killing the “own” cell.
The author of this study at the University of Texas MD Anderson Cancer Center researched the role of NK cells in the immune system’s ability to recognize its “own cell”. As a cancer cell is dedifferentiated, it loses the property of recognizing that it belongs to its own organism, so it is destroyed by the NK cell (through the absence of an inhibitory ligand).{*}{*}{*}
NK cells are abundantly found peripherally in the bloodstream, but can also be detected in several peripheral tissues, such as the lung.
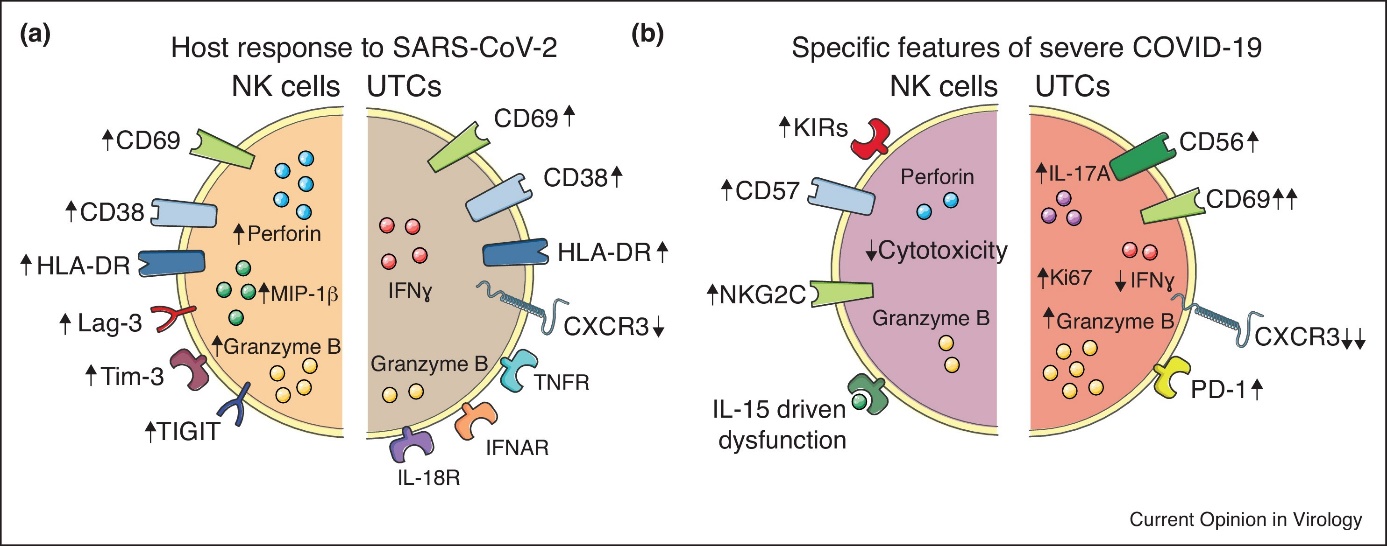
Figure 1.2. Phenotypic and function alterations in NK cells and UTCs in SARS-CoV-2 infection.
(a) The host response of NK cells and UTCs to SARS-CoV-2 infection is illustrated with modulation of surface receptors (arrows indicate change in expression) as well as intracellular effector molecules. (b) Specific features of NK cells and UTCs that have been associated with severe COVID-19. Taken from{*}

Figure 1.3. Innate and adaptive immune response in SARS- CoV-2 infection. The innate and adaptive immune response to SARS-CoV-2 infection. Hypothesis of the innate and adaptive immune response to SARS-CoV-2 infection. NK cells have direct killing effect on SARS-CoV-2 infected cells, as well as participate in antibody-dependent cellular cytotoxicity. Through inhibiting and activating receptors, NK cells recognize infected cells. Once activated, the degranulation of NK cells induces the releasing of perforin and granzyme which directly lyse infected cells. NK cells express CD16A, which participates in antibody-dependent cellular cytotoxicity. Meanwhile, NK cells also interact with dendritic cells in antigen presenting process and affect adaptive immune response. Monocytes can secret IL-6 that acts as inflammatory cytokine, resulting in the activation of other immune cells. Taken from ref. {*}.
To understand the normal, successful immune response to SARS-CoV-2 infection, the study of COVID-19 infection in children and adults with mild or asymptomatic disease is critical.
Following the same viral exposure, children have far fewer symptoms. As mentioned earlier, early, innate immune responses are more effective and pronounced in children, which is probably the key to rapid infection control and mild clinical infection.{*}
Let's look at the events of this normal, successful immune response point by point:
- NK cells appear robustly and contribute to the functioning of the early immune response in the presence of SARS-CoV-2
- NK cells are able to activate the immune response at distant points in the body via a chemokine pathway
- The NK cell recognizes the infected cell through its activation and inhibitory receptors, thus activating it, emptying the inclusions containing perforin and granzyme, killing the cell through lysis.
- The NK cell activates the adaptive immune response by CD16A surface expression, thus eliciting antibody-mediated cytotoxicity.
- Meanwhile, by chemically attracting other members of the immune system, especially dendritic cells, it accelerates antigen presentation toward the adaptive immune response. {*}
Now let us see how the immune response differs in COVID-19 infections with severe or fatal course. In these conditions, COVID-19 infections have been shown to inhibit NK cell function, leading to an imbalance of the physiological innate and adaptive immune response. Aging and other comorbidities are a clear risk factor for this.
- NK cells circulating in the bloodstream migrate en masse to the lungs, depleting these circulating populations and contributing to lung tissue damage
- The concentration of the macrophage-associated IFN immune response is high in mild diseases, while early high levels of IL-6, IL-10, IL-1ß were measured in severe infections
- Cytokine storm and “direct interaction of viruses” prevent the cytolytic effect of NK cells
- Exhausted NK cells are unable to effectively lyse infected cells, thus preventing an uncontrolled release of cytokine from infected cells
- Neutrophil granulocytes cause tissue damage and thus complement cascade activation, which can have fatal immunothrombogenic effects in the lungs and kidneys
- Monocyte HLA-DR (human leukocyte antigen) expression and neutrophil granulocyte activation, which represents an offset ratio relative to lymphocytes, are good biomarkers for the outcome of infection in high-risk patients
- The virus directly activates macrophages and CD4 + T cells that contribute to the cytokine.
A recent in vivo study highlights the difference in upper-lower airway virus-host interaction that determines the outcome and pathogenesis of SARS-CoV-2 infection. The role of the nasal mucosa in viral transmission and immune defense may allow for early interventions. NK and macrophage cells of the innate immune system are recruited at this site during infection and are involved in this first-line protection.
Abnormal cytokines storm lead, if the NK cells of the innate immune response at this site do not function properly and the aforementioned IFN-1 levels begin to rise only late.{*}
It also leads to a pathological cytokine storm if the innate immune response in the lower respiratory tract, i.e. the lungs, is activated early, which is the pathophysiological basis for uncontrolled late lung damage.{*}
Thus, dysfunction and delayed response of the innate immune response characteristic of severe COVID-19 infections {*} and the predominance of an overactivated, depleted immune response, the main drivers of which are the release of uncontrolled inflammatory cytokines and the activation of monocytes.{*}
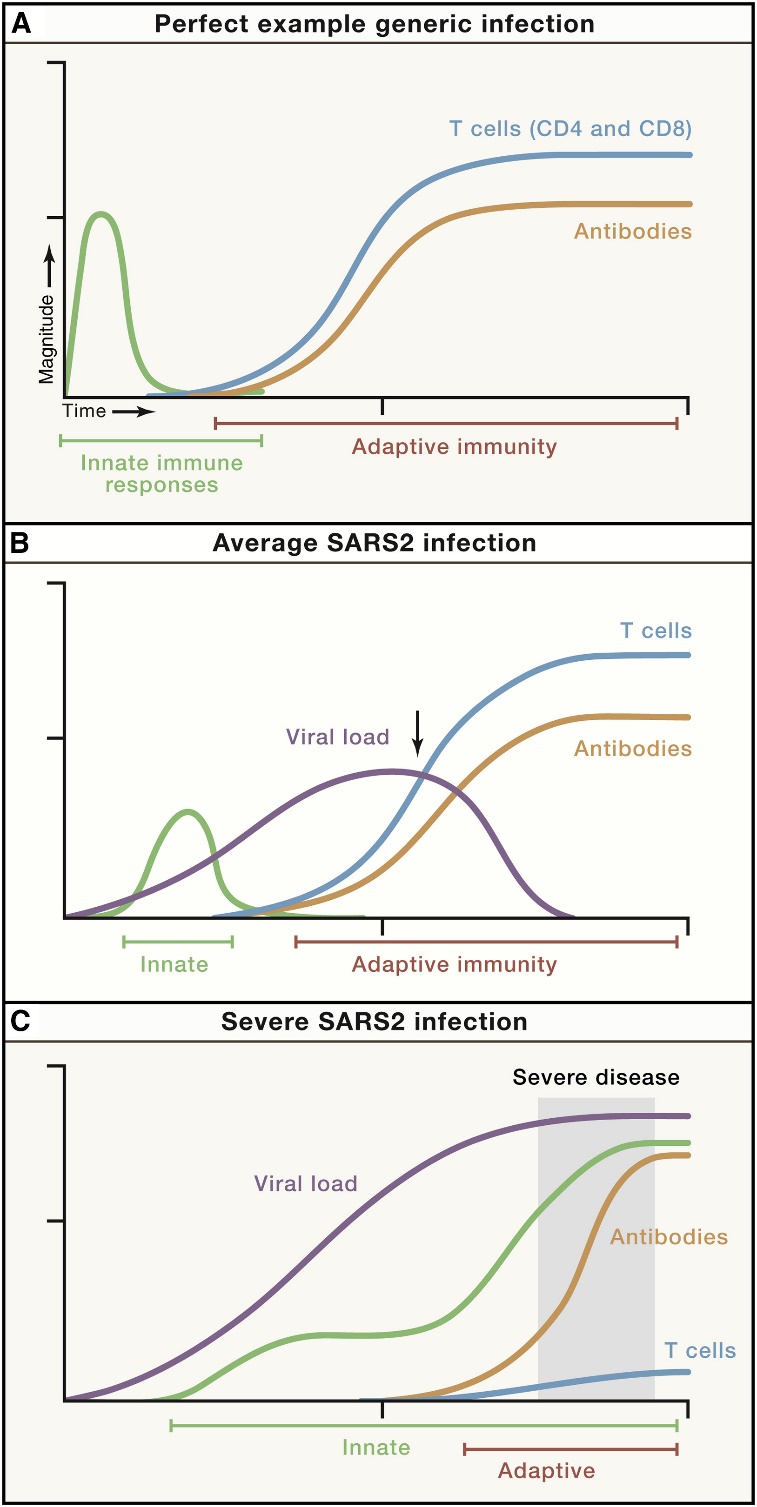
Figure 1.4. An integrated working model of COVID-19 immunology and disease severity. Immune response trajectories in COVID-19. Conceptual schematics of the kinetics of immune responses to SARS-CoV-2 under conditions of average COVID-19 (non-hospitalized cases) and severe or fatal COVID-19. “Innate immunity” line specifically refers to the peak kinetics of innate cytokines and chemokines detectable in blood; innate immune responses occur locally throughout the course of an infection. “T cells” refers to virus-specific CD4+ and CD8+ T cells. “Antibodies” refers to virus-specific neutralizing antibodies. Arrows indicate a time point with important differences in the presence or absence of T cell responses and the magnitude of the viral load, comparing (B) and (C). (A) An example of a generic viral infection. (B) Average SARS-CoV-2 infection. (C) Severe or fatal SARS-CoV-2 infection. The period of severe COVID-19 clinical disease is shaded gray. It is noteworthy in Figure A that, in the case of well-functioning local innate immunity (children and young adults), the virus appears almost systemically as it is already locally eliminated.{*}
It is essential to study the initial, organizing role of NK cells in SARS-CoV-2 infection for more effective, innovative immunotherapy in the future.{*} {*}
The author of the study and colleagues at the MD Anderson Cancer Center have studied the behavior of activated and inhibited NK cells ex vivo and in vivo.{*} {*} {*} {*} {*} {*}
One possibility is to use IL-10-producing NK cells programmed in NK cell immunotherapy or NK cells involved in the inhibition of the NKG2A / HLA-E signal line. Thus, cytolytic NK cells can prevent cytokine storm by reducing viral load.{*}
Although rare in children (1/1 million under the age of 18) with systemic COVID-19 (multisystem inflammatory syndrome in children- MIS-C) with severe course, elevated inflammatory markers and fever, where the disease leads to a clinically severe infection similar to adults or Kawasaki-like immune vasculitis, however, in these cases the immunobiological markers (autoantibodies, T cell types) correspond to the immune profile seen in autoimmune diseases.{*} {*} {*}
Consistent with the remarks in Chapter 2, we also describe here that these children at risk for developing MIS-C should be vaccinated according to British and Swedish models.Due to the fact that SARS-CoV-2 vaccines are currently administered intramuscularly, the immunization they induce bypasses the otherwise physiological, nasopharyngeal pathway.
It is a logical assumption that mucosal vaccination mimicking physiological conditions may lead to more effective immunization, so it would be worthwhile to develop this immunization strategy in the future.{*}
Unlike our skin, the mucous membranes, due to their permeability, are excellent surfaces for infections. This includes the gastrointestinal tract, the mucous membrane of the upper and lower respiratory tract. For this reason, the human body has developed a mucosal immune system that provides first-class protection against pathogens. Secretory IgA plays an essential role in protection and effectively inhibits the systemic invasion of pathogens.
Surprisingly, vaccines, largely bypassing this pathway, are designed for intramuscular administration, thus playing a protective role in the second-stage systemic invasion.
Thus, these “systemic” intramuscular vaccines cannot intervene in the initial mucosal infection at the time of a given pathogen, but have other disadvantages: since the use of a needle is essential, local needle damage, infection, poor administration of the needle (eg fat ), there is a need for reduced compliance and medical staff in children, as opposed to mucosal immunization (intranasal or oral administration e.g.
The same can be seen with the SARS-CoV-2 vaccine, where the vaccine bypasses the mucosal immune system, both through injection beyond natural mucosal barriers and through the artificial configuration of RNA-containing nanoparticles.
Recently, several studies have shown that nasal spray can also be an effective vaccine.{*}
Figure 1.5. Studies related to the development of nasal vaccines. in the middle of 2021. Taken from ref.{*}
Based on the fact that SARS-CoV-2 is also a respiratory virus, a higher level of mucosal immunization is presumably required to slow or inhibit the transmission of the virus.
The most effective pathway in population-level virus protection is probably mucosal immunity, which allows the formation of anti-SARS-CoV-2 S-IgA and TRM cells on the nasopharyngeal surface at the first point of contact with the pathogen, immediately inhibiting mucosa, viral replication, colonization, and thus the spread of the virus to the lower respiratory tract.{*}
Experimentally, a single-dose nasal spray vaccine against SARS-CoV-2 packaged in adenovirus protects against infection in the upper and lower respiratory tract of rhesus monkeys.{*} In addition, by ensuring the mucosal presence of TRM cells, mucosal vaccines can protect against the development of mutations that are no longer affected by circulating SARS-CoV-2 IgG.{*}

Figure 1.6.. Shows mucosal and systemic immunization of nasal vaccinations in the upper and lower respiratory tract. a) The protective NALT is seen, where an IgA antibody-mediated immune response, mainly generated by the interaction of pathogenic and mucosal epithelial cells, develops. b) illustrates the function of BALT, where the humoral immune response predominates. Abbreviations: CTL, cytotoxic T lymphocyte; DC, dendritic cell; NK, natural killer; TCR, T cell receptor. Taken from ref. {*}
Worldwide, the combination of mucosal and parental vaccination has been shown to be effective against pathogens such as immunization against polio, influenza, and rotavirus infection.{*} {*} Mucosal vaccination also elicits a strong systemic humoral response that can neutralize pathogens that break through the mucosal barrier. Several studies are currently underway on mucosal vaccination for SARS-CoV-2.{*}
Studies show that intranasal immunization, through the mucosal IgA and T cell response, effectively neutralizes SARS-CoV-2 infection in both the upper and lower respiratory tract, and reduces the risk of mucosal vaccination, the primary site of virus inhibition at the site of infection. there is also the development of an antibody-dependent disease enhancement (ADE). {*}
The mucosal and systemic immune response elicited by mucosal vaccination, due to its easy and possibly cheaper application, may accelerate the development of herd immunity by mass vaccination, especially in developing countries, and may provide an easy self administered non-invasive vaccination option for patients. This also increases efficiency and speed by eliminating the need for a number of other requirements (such as the logistics challenges of transporting and storing the vaccine) {*}
The benefits of mucosal vaccination on a point-by-point basis are as follows:
- higher patient compliance
- patients can inject themselves, which reduces the need for and cost of medical staff involved in mass vaccination
- strict hygiene principles do not have to be observed during application, making it easier to store vaccine products
- eliminate needle-related complications (infection, vascular injury)
- greater capacity for mass extinguishing
- does not cause religious or cultural complications (the needle in some religions disturbs the sanctity of the body)
- antigen-specific sIgA and IgG are generated mucosally and systemically
- elicits an immune response at the primary site of natural infection that greatly reduces transmission{*}
Studies in the nasal mucosal infection model can be employed to assess the impact of viral evolutionary changes and evaluate new therapeutic and preventive measures against SARS-CoV-2{*}
Question 4 of our study arises: what is the rationality in that if the immune response in children is primarily provided by the innate immune system and the muscular, by pass vaccination is targeted basically the adaptive immune system, which is in children not the first really effective defense system?
It is of paramount importance that the provision of measures and physical protection for those over 60 years of age also allows the at-risk Elderly Population to refuse vaccination for younger generations, especially those under 12 years of age, for a number of reasons:
- On the one hand, the possible non-immediate negative effects of current and developing vaccines (ADE, myocarditis) cannot be ruled out with certainty.
- Based on current scientific findings, there is a chance that such adverse events may occur.
The growing unusual contagiousness{*} and disease severity of the newer and newer mutants of the SARS-CoV-2 raises the possibilities of the genetic modification and lab leak of the virus. The letter published in Science (2021) by outstanding scientists argued that the lab leak theory must be taken seriously and should be fully evaluated.{*} Recently, the first author of them stated, that „„the origin and early spread of SARS-CoV-2 remains shrouded in mystery”{*} The House Foreign Affairs Committee Minority Staff Final Report listed a vast amount of evidences of the genetic modification and lab leak of the SARS-CoV-2 causing the COVID-19 Global Pandemic.{*} {*}
Virologist Juliet Morrison is researching the virus's "gain of function", where further studies are being carried out to analyze the spread and infectivity of a pathogen. These studies have also raised the question of the origin of SARS-CoV-2. {*}
To produce the mRNA vaccine, additional genetic modifications were made to the region encoding the spike protein to protect the mRNA from early degradation after administration, with the mRNA region being more similar to human mRNAs, making translation more efficient antigen, i.e., the formation of the spike protein.{*} {*} {*} {*} {*}
Merck CEO Kenneth Frazier warned us that the speed of vaccine development is “causing serious harm to public health”.. Vaccinations must be supported by rigorous, scientifically based results, as previous examples, such as swine flu, “do more harm than good”.. It is not entirely clear how the virus affects the immune system and therefore how the vaccine will interact with the human body. "Ultimately, if we use the vaccine on billions of people, it's good to know how it works." {*}
A similar warning publication was published with this {*} {*} and potential Antibody-Dependent Enhancement (ADE) in Nature columns.{*} {*} {*} Other notices warn of appropriate due diligence.{*}
By altering the S1 subunit of the spike protein, cell signaling is altered and ACE2 is suppressed.{*}
Spike protein-like S1 proteins (S1 protein-enveloped pseudoviruses without viral RNA) damage and prevent mitochondria in human endothelial cells in in vitro studies. In addition, in an in vivo experiment, high blood pressure was induced in Syrian hamsters through the ACE2 dowregulation mentioned in the previous paragraph.{*}
Because SARS-CoV-2 carries immunogenic epitopes that are similar to human proteins, the issue of autoimmunity arises as a complication{*}, which was also emphasized in the Charite in Berlin through biomimicry.{*}
Antibodies formed by the spike protein have so far cross-reacted with 18 endogenous tissue antigens (eg liver, mitochondria, nervous and gastrointestinal tract, pancreas).{*} In another study, 26 identical heptapeptides between human endogenous protein and spike protein were identified.{*} Thus, the spike protein can cause autoimmune diseases after SARS-CoV-2 infection, and even the risk of developing autoimmune diseases increases with mass vaccination, especially in those who are predisposed to it.{*} Guillan Barré syndrome has been reported following Astra Zeneca and Janssen vaccinations.{*} {*}
Robert Jaenisch (Whitehead Institute) and other renowned scientists from NCI and MIT have pointed out that DNA copies of the SRAS-CoV-2 virus can be incorporated into the human genome. Thus, exogenous SARS-CoV-2 RNA, incorporated into the human DNA genome, allows the production of viral protein.{*}
In accordance with Brandolini's law, several scholars have questioned Jaenisch's findings,{*} however, in their responsive response, they demonstrated strong evidence for genomic incorporation of SARS-CoV-2 DNA and subsequent tissue expression in patients,{*} they also drew attention to studies with similar results.{*}
Regarding vaccination of children, based on our previous study, we summarize the rationality of vaccination if ..
… Death among children, long COVID is extremely rare and they can spread the virus whether they are vaccinated and / or unvaccinated?
… The primary and well-functioning defense mechanism of children is the innate immune system and vaccination in children is mainly aimed at the immature adaptive immune system, in addition, vaccination also bypasses the mucosal barrier, the natural immune system of the mucosa?
… Based on our current scientific knowledge, it is likely that autoimmune and other diseases may develop years later in mothers who have been vaccinated with the mRNA vaccine, as the vaccine is essentially an RNA-containing nanoparticle with an artificial configuration.
Analyzes demontstrate that the development of herd immunity to COVID-19 is almost impossible.{*}
The spread of infection is further enhanced by the higher transmission dynamics of new mutants and / or their ability to induce a large number of re-infections inherent in avoiding an immune response.{*} According to experts the immune threshold of the herd can rise up to 90%. Assuming that the overall efficacy of vaccines, especially mortality, is 90%, 100% of the population should theoretically be vaccinated.A prerequisite for the development of herd immunity is that the immunized individual no longer transmits the infection to the few susceptible individuals around it, so herd immunity should only be considered after the development of vaccines that prevent viral transmission. The questions are raised about the effectiveness of the repetitive booster vaccines. {*} {*}
None of the vaccines approved to date have shown how well they prevent infection or reduce the spread of disease in a population. Especially in case of Omicron. Memory responses to SARS-CoV-2 obtained with the present vaccines may alleviate symptomatic disease or limit viral shedding, but especially concerning the latter we have no idea how to exactly determine.
This is made even more difficult by the fact that the ever-emerging new virus mutant configurations rewrite the conditions over and over again. The conditions could be more complicated with other biological factors. For example, a robust memory T-response in the lung can limit infection and potentially reduce clinical symptoms by eliciting a complete systemic immune response while still allowing the virus to spread for some time, possibly from other mucosal surfaces (e.g., the nasal passage).
This leaves open the possibility that vaccines will remain susceptible to asymptomatic infections - and pass this infection on to others who remain at risk. Griffin: "In the worst case, people will be vaccinated who, while having a good time, are increasing the number of people spreading the virus unnoticed." {*} {*}
As early as 2020, Lipsitsch projected the above fact: "The worst case scenario is if there is a vaccine that relieves symptoms without reducing a person’s infectivity, which can even go backwards, as it makes those infected less careful and thus increases the spread of the virus." {*}
This logically leads to the fact that in some populations the number of COVID-19 PCR positive cases is independent of the degree of vaccination of that population. {*}
Numerous studies in non-human primates suggest that current parenteral vaccines in humans protect against severe COVID-19 infection but do not prevent upper respiratory tract infection. {*}
Natural SARS-CoV-2 infection provides better protection against reinfection than parenteral vaccination, as the former induces immunization at the site of infection in the upper respiratory tract. Thus, upon re-exposure to the virus, the pathogen first encounters a mucosa immunized with SARS-CoV-2, unlike the mucosa of a vaccinated individual. In mouse experiments, mucosal tissue memory T cells played an important role in such reinfections. Primates have already been successfully immunized with nasal spray (which better mimics the route of natural infection and thus immunization). These include nasal spray vaccines that produce dimeric IgA antibodies on the mucosal surface against SARS-CoV-2{*}The emergence of a mutant identified as Omikron from the dwindling Greek alphabet in the Spike protein, a preliminary analysis, was also shocking news worldwide. About 30 mutations can be identified, along with the re-emergence of several old mutation molecule configurations.
Threshold levels of herd immunity are estimated to be significantly higher since January 2021. In 2022 it can be around 90%.
The reasons for this are as follows. On the one hand, the significantly higher transmission dynamics of the new mutants (in case of Delta: R0 = 6 and HI = 84%), on the other hand, the ability to bypass the immune response, and on the third hand, a significant percentage of vaccine-refusing and hesitant populations (about 10-20% of ppl). This in itself and many others{*} vaccination alone cannot solve the level of protection for the entire population.
According to the LSHTM study, B.1.1.7. variant (alpha alpha) is 43-90% more contagious than its predecessor, but has not seen clear evidence of a change in disease severity, although increased transmission results in a higher incidence and more hospital admissions. {*} Harvard group data also demonstrate that SARS-CoV-2 variant B.1.1.7 may cause longer infections compared to non-B.1.1.7 SARS-CoV-2 (13.3 vs. 8.2 days). , which results in B.1.1.7. people infected for a long time can infect a larger number of contacts. Therefore, this extended period may contribute to the enhanced portability of B.1.1.7 SARS CoV-2.{*}
Even more dangerous are the Brazilian (Gamma, P.1 and Zeta P.2), Indian (Kappa B.1617.1 and Delta B.1617.2) and mu (μ) variants, also known as (B.1.621) spread worldwide, most recently Delta Plus (B.1617.2.1 or AY.2).{*}
Antibodies produced against previous variants and even bypassed. The new phenotypes may be associated with an increase in transmissibility therefore appear to be much more contagious. In addition they bypasses the antibodies produced against previous variants. This way they acquired the ability to re-infect by breaking through the previously acquired immune shield. This caused a chaotic situation in Manaus, where 76% of the herd immunity developed against the previous Wuhan tribes was also broken to such an extent that deaths were higher than during the first wave.{*} {*}
The Brazilian P1 mutant is particularly instructive. The mortality rate in May 2020 dropped to zero in September. This is explained by the development of herd immunity in the population due to 76%.{*} However, the hopeful situation was overridden by the new mutant (P1).{*}
Concerning the Indian (Kappa B.1617.1 and Delta B.1617.2) mutants, the sixth paragraph of the 89th SAGE meeting memorandum in England stated: “Indian variants are more contagious than B.1.1.7. variants". {*} Moreover, British Chief Medical Officer Chris Whitty acknowledged in this regard that “the Indian mutant is more likely to be more than 200% more contagious than the original Wuhani tribe”. In this case, the Indian version could lead to up to 1,000 deaths a day and 10,000 hospitalizations a day until the summer.{*} In Seychelles, where 86% of the population has been vaccinated, one-third of new infections have already been vaccinated and tested positive for Covid-19 in 2021 May{*}. When the mass vaccination in developed countries took place and the proportion of those immunized naturally reached a high value, Omicron came, creating deceptive positive perceptions about the future due to mild-onset diseases. However, the study released by the CDC in May 2020 is quite disappointing.

Figure 1.7. A CDC study showed nine deaths per 1,000 cases during the Omicron surge, compared to 13 deaths per 1,000 cases during the Delta surge and 16 deaths per 1,000 cases during last winter’s deadly surge.{*}
Seeing the above data, Fauci’s previous assumption that the immune threshold for the herd could rise to as high as 85% was amply met. The latest wave raging in Europe from November 2021 again and again overwrites the previously predicted “worse case scenarios”.
Like multidrug-resistant bacteria, mutant viruses that survive in immunized patients are prevalent due to selection pressure. Thus, vaccines inevitably lead to this, which is aided by convalescent plasma therapy and a significant number of mutations in individual immunosuppressed conditions that reduce susceptibility to neutralizing antibodies.{*}
“For the first time, mass vaccination campaigns are putting tremendous pressure on SARS-CoV-2 and providing more opportunities for new virus strains that can bypass immune protection. We have never seen a virus under such selective pressure, so we do not know how they will react." {*}
A COVID-19 vaccine that produces an antibody complementary to 1 antigen can easily trigger a single viral mutation. Cocktails of monoclonal antibodies, each capable of recognizing multiple regions of the spike protein (i.e., multiple antigens), may reduce the likelihood that such a mutation will be favored through natural selection, demonstrating the primacy of the body's natural immune response to elicit many antibodies.{*} {*} {*}
A rapidly developed vaccine could provide an opportunity for the development of unpredictable mutant variants of the virus in the future. {*} Future vaccines should be developed. {*}This further reinforces the ELSE strategy as isolating the Vulnerable Population by avoiding unnecessary deaths makes it possible to “wait” until a properly functioning cocktail or other version is developed.{*} {*}
Multispecific T cell responses elicited by natural infection provide multilevel protection, reducing immune bypass mechanisms.{*} A patient with COVID-19 infection shows a robust CD4 + and CD8 + T cell response to a variety of SARS-CoV-2 viral proteins, including S, membrane (M), nucleocapsid (N), and non-structural proteins (NSP). Assuming that memory T cells develop from these, providing a platform for enhanced and accelerated generation of new B-cell responses against viral variants.{*}
In contrast, most SARS-CoV-2 vaccine developments target the Spike glycoprotein, which can avoid the human immune response.{*} {*} Altmann Imp. Coll: "It will be necessary to be ready for other vaccinations if resistance to Spike vaccines develops."{*} A series of uniform mutations along haplogroups A and B may make it difficult to develop future vaccines.{*} By this logic, the combination of different vaccines may accelerate the immunization of the herd by enhancing the immune response.{*}
"Continuous monitoring and continuous sampling and sequencing are key to assessing potential effects on public health and detecting possible mutations, as well as ongoing research into the development of the next generation of COVID-19 vaccines."{*}
Of note is the study, which aimed to produce mutations with spike proteins that allowed antibody recognition to be avoided and were resistant to antibodies taken from the blood of humans recovered from COVID-19, as well as resistant to “monoclonal” antibodies developed for therapies.{*}
To prevent the mutation and consequently the virus from circulating for decades, it is still possible to eradicate SARS-CoV-2 using ELSE. According to the author, we are approaching 24 o'clock in terms of the possibility of completely eradicating the virus. It would be useful to have a systematic, comprehensive, coordinated master plan at the same time as developing a vaccine that is certainly effective in eradicating the virus. The main concern with the virus is the mutation.In principle, a vaccine that is perfectly organized and distributed globally can eradicate COVID-19 infection. Unfortunately, we can only talk about this in theory.
On a practical level there are many obstacles (from infrastructure, public health, communication related to vaccination), which depend not only on the amount of vaccine purchased in a given country as well as the allocation and efficacy of vaccines that can be planned, taking into account also the developed natural immunity.{*}
The increasing threat of new mutants {*} with higher transmission dynamics (Delta: R0 = 6) {*} and the ability to break individual immunity developed by previous variants and/or vaccines has raised the required protective herd immunity (HI) level to 90%..
This level cannot be achieved by vaccinations alone, but also by the natural immunity of the population, as emphasized by Allyson Pollock, a professor at the University of Newcastle. He also stressed that because of the length of immunity, the effects of the new variants, and the fact that the people are exposed to transmission and reinfection despite immunization, the new UK health secretary (Sajid Javid) could do his best for society when the strong restrictions, school closures were lifted.{*}
According to Sajid Javid, "although the number of cases will increase and many people will pay attention to proper hygiene and distance by reducing restrictions, we need to be aware that there will be no day in the future where we can do this without risk." - ie a reduction in restrictions- "Previous epidemiological restrictions have led to shockingly high levels of domestic violence and psychiatric illnesses".
In a vicious circle devastated by Sajid that more and more mutants will be a threat to the VP again and again, they will be attacked with the same or higher mortality rate, what is the rationality of recurrent severe epidemic restrictions, school closures and healthy youth and vaccinating children?
If we say that this 40-55 / 10k VP will be vaccinated to such an extent that half of them can escape, then again only half will be able to escape with the appearance of the next mutant, thus leading to the extinction of the unvaccinated{*} VP. Therefore, physical protection, i.e. isolation, could provide an additional line of defense for the above long-term biological (vaccination) protection.The change in immune competence with advancing age, the so-called immunosenescence (4.6.3.), is due to changes in the immune system over time. Antibody responses to vaccines may decrease with increasing age.{*}
The efficacy of rapidly developed vaccines is currently unknown. Current vaccines have been issued under the 'emergency approval' protocol, so the primary endpoint of these studies and drug development trials has been symptomatic. It was not possible to determine the infectivity of the infected participants and, most importantly, the risk of death in the vulnerable population. This is because it would have made clinical trials more protracted.
A remarkable study shows that older adults are excluded from vaccine trials, respectively. Such exclusions limit the evaluation of efficacy, dosage, and adverse effects. In recently published paper related to clinical trials with COVID-19, there were only young age groups with few or no participants over 75 years of age. If the older age group is excluded from the vaccine trials, it will not be possible to evaluate the efficacy, titration dose, adverse effects etc. in the group most at risk by COVID-19.{*}
M. Ostermann: "In order for vaccination to truly have a maximum effect, it must also reduce serious illness and death. We do not yet know whether it works in the most vulnerable elderly population at risk"{*} Krammer: "If enough participants from such elderly groups were included in the study, it would be possible to determine the effectiveness of the vaccine developed for them". {*}
Even before the onset of mutants, a study of four million in Denmark found that the natural protection of previously infected individuals was low among older people (80% vs. 47%).{*} That is why their protection (ELSE) is particularly important.We would recall the thoughts of Allyson Pollock (1.8), who emphasized the importance of immunity acquired through natural infection in addition to vaccination in the development of herd immunity, as the latter is long-lasting, probable life long. In addition to the already described disadvantages of parenteral administration, current vaccines focus on one epitope (spike). At least they should focus on the new epitopes created by newer and newer mutations, with the aim of developing specific antibody formation, even if it is related only one epitope. Inherently, natural immunity elicits a range of antibody or cellular immune response (T cell) against all immune epitopes of the virus, which explains the long-term, more mutation-resistant protection.
Evidence of persistent immunity is well available. Dispelling previous concerns that immunity to SARS-CoV-2 has been attributed to antibodies circulating in the bloodstream and that a decrease in immunity has been suggested, an article in the journal Nature on September 20, 2021 overwrites that patients with bone marrow from COVID-19 infection. In natural, mildly infected individuals, BMPC cells, in contrast to memory B cells, could only be aspirated from the bone marrow after infection, not from the bloodstream. Thus, these cells provide long-term protection in humans capable of producing robust antibodies.{*} For decades, antibody-producing cells have been identified that provide adequate immune responses, and their efficacy may be affected by viral mutations. Therefore, these patients are likely to be protected against SARS-CoV-2 virus infection for an unusually long time, even for the rest of their lives.{*}
In the bone marrow, these cells belonging to the humoral immune system that provide long-term immunity are BMPCs{*} (bone marrow plasma cells) and memory B cells, so these cells are authoritative for serological results when determining protection.
In infected individuals with a natural, mild course of the disease, BMPC cells, unlike memory B cells, could only be aspirated from the bone marrow after infection, not from the bloodstream. Thus, these cells provide long-term protection in humans capable of producing robust antibodies.{*}
The above immunoanatomical results are supported by several in vivo studies.
A large case-control study in Israel in August 2021 found that previous SARS-CoV-2 infection against the Delta variant provided greater protection against double-dose BNT162b2 vaccination in terms of disease severity and mortality.{*}
Another study in 2021 also showed that higher antibody levels develop after a single dose of mRNA vaccination (BNT162b2) in those who developed natural SARS-CoV-2 infection compared to those who had previously received double-dose mRNA vaccination.{*}
Based on data from an October 2021 article in the scientific journal Nature, a stronger immune response is expected in vaccines who have a history of COVID-19 infection.{*}
The key to sustained immunity is that the immune system targets multiple epitopes and antigens of the virus, and multiple antibodies are developed for this purpose. This phenomenon is basically based on the T-cell response.
By artificially infecting primates - Rhesus Macaques whose immune response can be considered almost identical to that of humans - naturally developed cellular immunity protected them from repeated exposure.{*} {*} {*} {*}
CD4+ and CD8+ T cells targeting multiple regions of SARS-CoV-2 are maintained in the resolution phase of both mild and severe COVID-19. (Fig. 4.) {*}
Peng et al. report a robust and diverse T cell response targeting multiple structural and non-structural regions of SARS-CoV-2, irrespective of whether the individual had mild or severe infection. While the most frequent responses were against peptides spanning spike, multiple individuals recognized membrane and nucleoprotein antigens, all eight regions tested. Such multispecific T cell responses are well suited to providing a fool proof form of multilayered protection, mitigating against viral escape by mechanisms such as mutation or variable antigen presentation.{*}

Figure. 1.8. Frequency and specificity of T cells in the resolution phase of mild or severe COVID-19. (Taken from Swadling et al). Peng et al. studied the resolution phase of COVID-19 (blue box), showing a broadly targeted CD4+ and CD8+ T cell response (cell colors and numbers represent relative frequencies of indicated protein specificities). The total T cell response (solid blue line) is stronger and broader in severe cases (assumed to have had higher viral burden, red curve), correlating with stronger antibody responses (solid gray line). However, there are, proportionally, more CD8+ T cells in mild disease. Central questions arising from this study (listed in red) concern the unknown hierarchy and kinetics of T cells (dashed blue lines) and antibodies (dashed grey lines) in the acute and memory phases.
In another study, which also showed a higher percentage of activated and proliferating CD8+ T cells in mild as compared to severe COVID-19, the SARS-CoV-2 elicits robust memory T cell responses, suggesting that natural exposure or infection may prevent recurrent episodes of severe COVID-19 also in seronegative individuals{*}
The SARS-CoV-1 (as designated in this paper since the various previous identification occurring in the literatures also “novel” coronavirus and/or SARS and/or SARS-CoV etc) infection could develop longer-lasting immunity and the beta-coronaviruses can induce immune responses against one another.{*}
Study demonstrated the presence of cross-immunity in humans, since an antibody, from 2003 against SARS-CoV-1 named S309, neutralized SARS-CoV-2 and SARS-CoV-1 pseudoviruses as well as authentic SARS-CoV-2 by engaging the S receptor-binding domain.{*} In other studies, the pre-existing SARS-CoV-2 cross-reactive T cell responses were observed in healthy donors, indicating some potential for pre-existing natural immunity in the human population.{*} {*}
These studies also verified the presence of SARS-CoV-2−specific, S-reactive CD4+ T cells in COVID-19 patients suggesting the possibility of permanent natural immunity that was proven previously with SARS-CoV-1 coronavirus existing more than six years concerning the CD4+T cells, even if the lack of CD8+T cells by that time.{*} Although in similar study, the CD8+ T cell responses were found to persist up to 11 years post-infection, targeting the SARS-CoV-1 membrane and nucleocapsid proteins.{*} Because SARS-CoV-2 and SARS-CoV-1 have 90% amino acid homology for nucleoprotein and 73% amino acid homology for receptor binding domain (RBD), serum from patients with SARS-CoV-1 might cross-react with SARS-CoV-2 immunoassay.{*}
The antibody response may decrease as a standard response to viral infections, {*} however, a recent study shows that antibodies to SARS-CoV-2 did not decrease within 4 months of diagnosis.{*} A recent study found that levels of antibodies to coronavirus spike protein decreased over six months, however, participants had constant levels of B-cells{*} in memory specific for the production of antibodies to spike protein and were able to remember and accelerate antibody production even when titer decreased.{*}
Future vaccinations against emerging coronavirus variants should emphasize the memory CD8 T cell response for optimal protection.{*} Importantly, SARS-CoV-2-specific T cells were also detectable in antibody-seronegative family members and in individuals with a history of asymptomatic or mild COVID-19 infection. {*} Recovered individuals developed SARS-CoV-2-specific IgG antibody and neutralizing plasma, as well as virus-specific memory B and T cells, which not only survived but in some cases increased numerically within three months after the onset of symptoms{*} and presumably thereafter.
According Altmann DM, from Imp. Coll., published in Science and Nature: SARS-CoV-2-specific memory T cells are likely to be critical for long-term immune protection,{*} and the virus appears to stimulate T cells.{*} The cellular immune response to SARS-CoV-2 was also found in COVID-19 convalescent subjects and neutralizing antibody titers correlated with the number of virus-specific T cells.{*}
Krammer demonstrated the convergent antibody response in a large cohort study.{*} {*} Also positive IgG or IgM confirmed COVID-19 infection in both symptomatic and asymptomatic patients.{*}
Further study found immunity of humoral and circulating follicular helper T cells to spike protein in recovered patients with COVID-19 {*} Antibody cocktail generated from recovered patients and humanized mice against spike protein SARS-CoV-2 prevents the ability of viral mutations to lead to antibody resistance {*} Antibody responses behave similarly not only for the spike but also for many other domains of SARS-CoV-2 antigens. Killer T cells show enhanced immunity to new mutants.{*} Killer T cells show enhanced immunity to new mutants killer T-sejtek.{*} All studies refer to the efficacy of innate immunity as a result of vaccine-acquired immunity, particularly with respect to the T cell response.
Evidence for the development of herd immunity in SARS-CoV-2 infections has become apparent in previous hot spots studied in New York {*}, Italy{*} , Mumbai, {*} and Brazil. {*} {*}
“It is impossible to stop the coronavirus. Let's protect older people because they die.” {*} Use the ELSE strategy to help protect the Elderly Vulnerable Population.The current state subsidy for empty hotel beds is also significant. There are many ways to calculate, but any calculation method shows that if the state takes over the costs of isolation, it results in significant savings, especially when analyzed on a project-by-economy basis.
According to the calculation (2.7.1), this is an even more favorable cost in itself than the cost of intensive treatment of those concerned.
In addition, state support, only for the tourism sector, remains significant, so the huge budget money paid by taxpayers to sustain the sector is not wasted, as it can even cover the costs of isolation.
Preventive intensive care alone costs for example more than physical protection (2.7.1) and the current state subsidy for empty hotel beds is significant. There are many ways to calculate, but any calculation method shows that if the state takes over the costs of isolation, it results in significant savings, especially when analyzed on a project-by-economy basis.
The calculations for the US and EU are well detailed in 2.7.1., but the results are closely similar concerning to Hungary for the ten million people. If, due to the epidemic, the economy has to be limited to 1 month in accordance with the current measures during the repetitive wave periods, the loss of HUF 15-20 billion per day to the state, ie HUF 450-600 billion per month. At the same time, 20,000 people out of HUF 50 billion a month can live in a 4-5-star hotel. The numbers speak for themselves and if the isolation would be implemented, there is no need to limit the economy, because the health system, through the measures described int he Introduction (small special „COVID-hospitals” parallel isolation etc), can provide professional and effective treatment of the rest of the population without restrictions. And the lives saved cannot be expressed in numbers.
The procedure would be essentially voluntary. Plenty of high-quality reception capacity is available and not only for 0.1–0.2% of unvaccinated vulnerable people, (2.7) but also for Hungary, for example, up to 2% of the population can command and manage defense work. Thus, the possibility of isolation is open not only to the VP who rejects the vaccine, but also to the VP who would receive a serious increase in morbidity and mortality (due to a reduced immune response, vaccine ineffectiveness, mutants, etc.). This represents a multiple safe buffer for 0.1-0.2% of the strictly designated unvaccinated VP. In this way, possible ethical problems can be prevented, such as setting a limit, exclusion, rejection, and so on. Once we have “practice” with this physical protection, we will be able to defend ourselves more effectively against the waves caused by this and other virus variants in the future, also contributing to the possibility of their final elimination.
Not to mention the real value. The value that worth infinitally more than the money:
- first of all, the lives saved, moreover
- the years of life lost (YLL){*} quality-adjusted life years (QALY){*}{*}{*}{*} and welfare years (WELLBY){*}
and the liberated sense of life through the restoration of socio-economic life.
New mutants caused by massive parenteral vaccinations are triggering new waves of epidemics, causing deaths to surge again and restrictions to be imposed again.
The most affected part of this working age in particular (restaurants, events, etc.) will be reluctant or unwilling to submit. This civil resistance will further pave the way for the further, more free and devastating spread of SARS-CoV-2. At the onset, or even in the middle, of vaccination, the population is susceptible to infection, and there is not yet adequate population protection, which is exacerbated in the elderly by a reduced immune response to vaccines, thus increasing mortality.
So the vicious circle above could, paradoxically, happen during the mass vaccination and claim more casualties from wave to wave. The situation could become unmanageable. The tension between the generations can go all the way to the extreme.
The dramatic process, which is accelerating in a short period of time, could place an unprecedented overload on the health care system that will not be able to compensate for the rate of vaccinations. This will increase mortality even further, the economy will slow down again.
Generational differences in vaccination-related attitudes and immune responses:
In the emerging vicious circle, intergenerational tensions could escalate to the extreme, with young people shocked to find that there will be a sizable number of seniors refusing vaccination.
The working age population has so far made this horrific sacrifice to protect the lives of the elderly. If these elderly people are unwilling to vaccinate themselves, how can young people be expected to make additional sacrifices, obedience? The only obvious solution to this situation is for society to offer the possibility of protection from physical isolation to the Vulnerable Population who refuses vaccination (0.1-0.2% of the total population).
Christian Drosten, a leading German epidemiologist, said that “the introduction of mass vaccination will put enormous economic, social and political pressure on the introduction of any necessary restrictions, which could soon lead to overloading the health system and a high number of deaths.{*}
It is difficult for ordinary people to explain the paradoxically high mortality rate and the additional restrictions required in the midst of ongoing vaccination. It will seem to people that the tragedy of the pandemic is steadily increasing in parallel with the vaccines, the vaccine is not effective enough.
Isolating the Vulnerable Population that refuses vaccination in a timely manner could avoid the high number of deaths and short-term unmanageable situations that would result in:
- Vaccination can be done in a reassuring manner
- People's faith in vaccination would be strengthened
- It would be more efficient to catch the slice from the sails of vaccination skeptics
- Moreover, once a “routine” has been mastered in the isolation technique, it would be easier to defend against mutants that evade the immune response.
- This would not force further or very strict closures
- Last but not least, accelerated transmission dynamics (R) would allow faster signaling in clinical trials
The primary endpoint of current vaccinations is the symptomatic response to the measures. They cannot determine the infection of the infected participants and, most importantly, the prevention of mortality in the vulnerable population.
Given the reduced compliance (4.6.2) and reduced immune response (immunosensitivity, 4.6.3) of the elderly, as well as the bottlenecks created by the production and distribution of vaccines, there is still a long way to go to develop protection at the population level, while creating a dangerous environment. for the VP.
M. Ostermann: "In order for vaccination to truly have a maximum effect, it must also reduce serious illness and death. We do not yet know whether it works in the most vulnerable elderly population at risk." {*} Krammer: "If enough participants from such elderly groups were included in the study, it would be possible to determine the effectiveness of the vaccine developed for them." {*} The Robert-Koch Institute does not recommend the administration of Astrazeneca to the elderly in Germany.{*}
Because the virus has the unique property of being dangerous to a well-defined and identifiable group of the population, it is necessary to isolate them during the waves until a suitable vaccine is developed for them. If they are excluded from development, it is a challenge to develop a suitable vaccine for them.The ELSE study, with a new approach and elaborated details of feasibility, proposes a solution to the expected difficult situation and shows that with careful professionalism and discipline it is possible to safely isolate this Vulnerable Population while offering and providing cultured, livable conditions as long as a sufficiently effective vaccine against the mutants are not being developed.
A unique feature of SARS-CoV-2 is that the virus threatens only one personally identifiable narrow Vulnerable Population (VP) with severe or fatal consequences, predominantly in the elderly and suffering from various chronic conditions (2.5). This is still true with the unfortunate proliferation of new mutants, where more and more young victims are occurring, but more than 90% are still characteristic of the aforementioned VP over the over 60s.
As the principle of the ELSE strategy, the study-– based on the CDC evidence lists (2.4.2.) - condensed the appropriate information from the relevant literature and statistics and concludes from them for the possible implementation of the safe isolation of the Vulnerable Population.
In the study, all of the significant meta-analysis and systematic review were carefully examined in order to define and compare the seriousness of the underlying diseases related to COVID-19, based on age, preexisting conditions, other health parameters (2.4.4.) and comorbidities (2.4.5.). Based on the guidelines and the score system (2.5.) set up from all of this information, the local health authorities and the GPs, - who personally familiar to them and to their actual status - would finalize the score system individually, resulting a surgically precise possibility of identification and isolation of the Vulnerable Population.
VP of patients at risk of needing intensive care accounted for only 1.4% of the population (144/10k, IFR 0.9%, R0 = 2.4) and half of these cases (72/10k). ) leads to death. Data were adapted from Imperial College Report-9 (2.6).
ELSE offers a solution to the epidemic that complements vaccination by being able to precisely isolate the vulnerable population that refuses vaccination (0.2%), thus also offering a better chance of eradicating the virus.
Additional reasons for isolating the Endangered Population:
- This will provide an opportunity to extend ongoing experiments to additional endpoints, involving the necessary subgroups and waiting for other vaccine developers to develop a vaccine that meets all requirements and expectations using cocktails, including death prevention.
- If immunity is not evenly distributed within a population, groups of susceptible hosts may remain that interact frequently. Even if the proportion of immunized individuals in the population as a whole exceeds the immune threshold of the herd, there is still a risk of local cluster-like outbreaks through these patches of susceptible individuals.{*}
The impossibility of isolating the Vulnerable Population has been entrenched in the mindset as an unshakable dogma. Skeptics doubt the that the basically elderly vulnerable population could really be protected. For them, such a superficial explanation is that several generations live under one roof, young people work in a nursing home, and so it is still sufficient to conclude that it is impossible to prevent infection. There is no carefully designed, scientifically developed and analyzed study in the literature on the safe physical segregation of vulnerable populations. And the opportunity to save tens of millions of lives would deserve at least one. Skeptics can only consider this conceivable that the entire elderly should be isolated. This would mean 20-30% of the population (3,000 / 10k), which is obviously impossible.
The inseparability of the VP has been fixed in the mindsets of sceptics as an ineradicable dogma and prevents any other approach to prevail. They consider it is necessary to isolate 20-30% of the population. Of course, it is not possible to isolate that many people, but it is possible to safely isolate the 0,7% (2.6.2) whose lives are in danger. They are identifiable (2.4 and 2.5), and can be safely separated (2.7).
Increasingly threatening new mutants{*} with higher transmission dynamics (R) and breakthrough immunity to previous variants justify the need to offer a level of isolation not only to the Vaccinated VP but also to the already vaccinated VP (VPCRH 2.7.1.).
Therefore, the analysis below continues to apply not only to those who refuse vaccination, but also to the entire Endangered Population (0.7%). The number to be strictly segregated is max 0.7% (72/10k) of the total population. Such a small population can, of course, be safely isolated by protocols systematically based on ELSE, compared to the huge population assumed by skeptics (3,000 / 10k).
Essentially, the procedure would be on a voluntary basis. There are plenty of high-quality capacities for isolation, not only for the 0,1-0,2% of non-vaccinated vulnerable people, but also for 6% of the population(2.7.1.), - providing a 30-60 times safer excess buffer for the 0,1-0,2% strictly designated, non-vaccinated VP - so there can be no ethical objection to the applicability of the isolation (limit, exclusion, rejection, etc.).
The isolation of the VP is independent of the constraints of the rest of the population. Decision-makers are free to choose according to epidemiological parameters, reduction or absence of ICU bed burden, mortality, intensive bed load, and actual progression of vaccination.
The mindset of skeptics as a dogma prevents any more purposeful, sophisticated other approach. They cannot think further about the fact that it is not necessary to isolate 20-30% of the population over the age of 60 (2-3 million/10 million inhabitants in Hungary). Of course, it would not be possible to isolate so many people, but only 0.7% (70,000 in Hungary 2.6.2) whose lives were really in danger before vaccinations and could be in danger again with the appearance of an even more aggressive mutant could be isolated. They can be identified (2.4 and 2.5) and securely separated (2.7). Within this, the rate of those who refuse vaccination is only 0.2-0.3% (10-20 thousand people/ ten million).Isolation of VP is not only justified but also morally fully acceptable based on:
- In the event of the next wave, the elementary protests of the young generation after the mass vaccination against the measures has begun will make it impossible for the appropriate level of restrictions to take effect.
- The new vaccines have not been shown to be effective in the mortality of the elderly.
- Furthermore, it is not clear whether recently approved vaccines prevent infection, the transmission of the virus.
- The elderly have reduced immune response. After initial infection, protection against recurrent infection was approximately 80%, but decreased to 47% in those over 65 years of age. New SARS-CoV-2 mutants (South African, Brazilian and triple-mutant Indian)
• not only an increase in higher transmission dynamics (R0), resulting in a higher herd immunity threshold,
• but also the breakthrough and circumvention of the previously developed immunity
• Thus, neither the current immunity of the herd nor the current vaccines can so far provide satisfactory evidence of adequate protection against new mutants.
• All this further justifies the possibility of isolation not only for the refusing VP but also for the vaccinating VP until safe population-level protection is established (through the development of a flock immunity and / or a suitable vaccine for them). - It is also ethically questionable to force a VP who refuses to be vaccinated to be vaccinated with various discriminatory provisions, as in addition to their own fault, they are too afraid of the side effects of vaccination until the effectiveness of vaccinations in terms of death has been sufficiently demonstrated.
- ELSE also demonstrates that isolation can result in up to a 10-fold safe buffer through available capacities for potentially fatal cases. Thus, we can also offer a chance to those who do not fall into the strictly defined category of VP but want to be safe due to age and / or less risky comorbidities, or simply fear of death (2.7).
- The segregation of the VP is independent of the constraints of the rest of the population.
- Connection is basically recommended on a voluntary basis, ensuring data security.
- For the management of those who would belong to the Endangered Population who refuse to be vaccinated but are unwilling to join, they must adapt to the necessary binding regulations in order to save their lives (3.8.2).
- Selection for the VP applies not only to the older generations, which corresponds to the vast majority of cases, but also to vulnerable minorities who may be in the younger age group (5.2).
- New mutants continue to attack the same VP with the same mortality rate. The observed “higher” mortality rate among young people does not significantly reduce the proportion of VPs that can still be identified and isolated. This observation cannot constitute a counter-argument against their isolation.
- One of the arguments for vaccinating healthy children and juveniles, which has been questioned several times in the introduction to our study, would be permanently discontinued, according to which VP should be protected from the presumed transmission of this age group.
A uniform level of adequate flock immunity should be formulated in conjunction with natural and vaccine-induced immunity, by further vaccination of those not yet infected on geographically white patches, and by leveling the level of herd immunity throughout the country. The quick test and scanning the QR code can help you with this. This makes it even more possible to identify and isolate those infected {*} from the remainder of the population and further reduces the dynamics of transmission.
Last but not least, we need to convince our fellow human beings in certain cultural circles to stop culinary delights like bat eating, especially with regard to Rhinolophus shamelit, {*} which is the source of a potential candidate for SARS-CoV-3.
The viability and reasonableness of rapidly developed and administered first-line vaccines may be questionable, as the primary concern is the prevention of deaths and serious cases that overload the health care system, rather than the protection of other asymptomatic or mild cases from infections.
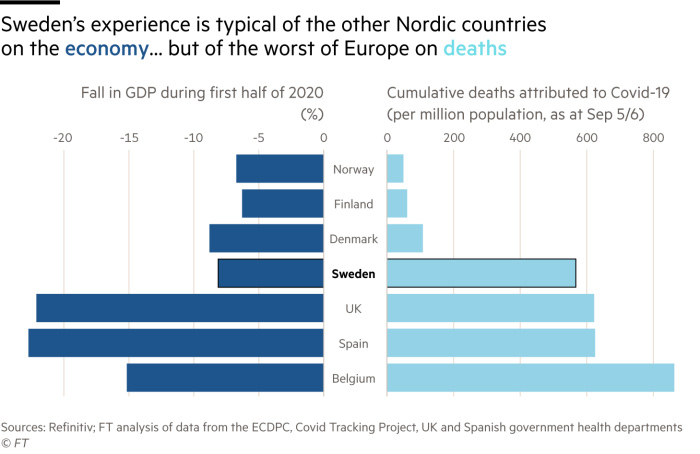

Figure 1.9. Situations in Sweden in 2020 in terms of key economic and mortality indicators. The image on the right illustrates the Swedish method used at the time of the outbreak. “ The introduction of the vaccine will not necessarily solve all the accumulated problems at once. Simple solutions to complex problems will not be easy.” {*}
Anders Tegnell has protected his country from the trauma of restrictive measures. Young people were able to complete their studies without school closures. The working age group has also been able to work and live their lives, as a result of which the economy has suffered the least during the epidemic period compared to other countries, and DALY, QALY, WELLBY figures in these younger generations are much better than in the EU and US. Deaths have remained well below the European average and have basically only occurred in the elderly Vulnerable Population, which will sooner or later be overtaken by the virus if they are not physically protected during the waves.
Two years later (2022 05 23 IHME), the cumulative mortality rates per 10 million inhabitants were as follows:
| Norway: 5708 | Finno.: 7813 | Denmark: 10800 | Sweden: 18485 |
| UK: 29133 | Spain: 25422 | Belgium: 27833 | Europe: 26446 |
The main elements of the success of the Swedish method were:
- economic and social life should not be paralyzed by drastic measures (especially school closures)
- the use of masks in more crowded places (restaurants) during the waves, the absence of mass events at the top of the waves, the restriction of the opening hours of bars
- mass communication focused on people perceiving the essential elements of curbing the epidemic and applying it involuntarily in all situations (social distance)
full compliance with official measures (especially with regard to the distant behavior of the elderly and the distancing attitude of the young generation towards the elderly, imbued with similar protective, respectful responsibilities) - Unconditional respect, compliance, and commitment to leaders
- Cultural habits have contributed to the success of the epidemic (eg they are located far away from each other in public transport, regardless of the epidemic, and many elderly Swedes live alone in small flats)
The Japene method:
Japan's constitution prohibits strict closures, (!) So a different strategy was needed to curb transfers. This has led Japanese society to follow and adhere to the so-called “3C –sanmitsu” (Closed environments, Crowded conditions and Close-contanct settings) rule, ie to avoid closed environments, crowded conditions and close contact. Japan has widely promoted this concept and urged people to avoid high-risk activities such as karaoke bars, nightclubs and indoor dining. People largely complied. A jury of artists, academics and journalists in 2020 chose sanmitsu as the slogan of the year in Japan.
Professor of Virology Hitoshi Oshitani, a Japanese government adviser on the pandemic, said in this year's Nature columns: “.. Terms often used such as“ exit strategy ”or“ return to normal wheeling ”. But we are nowhere near back to normal. Nations must continue to strike the best balance between reducing transmission (suppression) and sustaining social and economic activities. How? By minimizing suffering around the world using all available tools for cultures, traditions, legal frameworks and existing practices. There is no perfect solution to curb the epidemic, but careful study and communication is essential… ”.{*}
Japan's current cumulative death rate per 10 million population (IHME 28 May 2022): "only" 12,674.
In fact, all aspects of Swedish and Japanese “epidemic management” are aimed at isolating the elderly Vulnerable Population from potential virus sources as effectively as possible in order to reduce infection. Accordingly, both examples show that, in line with the ELSE VP strategy, isolating the Endangered Population and treating intensive cases rather than scattered, the root of the problem is solved, preventing any further negative consequences for society as a whole able to work and study.
It is also a fact that the Swedes also introduced stronger restrictive measures during the third wave than before. The author is of the opinion that the most effective epidemic management strategy is ELSE.
This cyclical supression methods during the waves used so far would have led to a similar result, but much less burden to the socioeconomic, if the authorities had imposed a strict, total ban on escape for only a five-day period (curfew) at the very top time of the epidemics wave for a short time. For those who are still in the initial latent incubation stage of the virus but are contagious, their infectious status would be revealed by the onset of symptoms during these five days. They and their direct contacts would be required to comply with normal quarantine. After that, life would only continue with the usual restrictive measures only in a limited time. However, it would quickly turn out that the number of new cases would fall spectacularly and the wave would go down much sooner, as the possibility of free movement of the main driver of the spread (super-spreaders) would be stopped. After the five days this asymptomatic super-spreaders and of course other “normal” spreaders would turn to be symptomatic and then could be easily identified and quaranteed.
Of course, even after this initial five-day period, there are asymptomatic people who also infect the others. However, their importance in relation to all transmissions to the population compared to super-distributors (4.6.6.) and those with specific symptoms is not significant. This is especially true for children and young adults in 1.2. as described in this chapter.
The five days could be solved by adding three days to the weekend, before and after it was announced in advance. In order to reduce absenteeism, certain mobile holidays, such as 1 May, could be scheduled here or 1 May could be declared a working day. If you are just about to triple or quadruple, Easter, Pentecost can be matched even more favorably in terms of downtime.
Decision makers and authorities have two options; they risk the aforementioned scenario, which is likely to lead to an unmanageable situation, or propose a new, different version, meaning ELSE with the segregation of the VP, which normalizes the atmosphere on all fronts and prevents social upheaval. As a result, tensions between the old and young generations of society are easing and the pressure on scientific life is easing.{*} {*}. Decreased compliance is difficult to eliminate quickly because it requires a long campaign {*} (4.6.).
The mortal effects of the vaccines that are being developed are currently unknown, and it would be extremely unethical not to allow the VP to refuse vaccination by offering live isolation due to the reluctance and immunosenescence of vaccination. It is still much more lucrative for the state to isolate VP in cruisers, resorts, and hotels than to pay for the consequences — not created by the VP — by suffering and sacrificing their lives in the intensive care unit. Based on a well-founded calculation (2.7.1), this is still a more favorable cost than the cost of intensive treatment of those concerned. Not to mention the lives saved and the tremendous benefits and liberated feelings of life through socio-economic recovery.
With these options in mind, the ethical, fair, and morally victorious attitude of decision-makers is to offer theVulnerable Population the option of voluntary holiday-level isolation, whether they are reluctant to be vaccinated or are already vaccinated.
Consequently, both the old and the new generation of society will be grateful to decision-makers who are able to make the right decisions and through isolation (VPCRH 2.7.1) can be a win-win solution.
All of these have been summarized to define the identification and selection criteria for members of the Vulnerable Population, which are summarized in the 2.5 scoring system.
For those who choose isolation:
- They can comfortably wait for the herd immunity to provide protection at the same time
- They can wait to develop a combination of vaccines that prevent death and then return to their homes and communities
- Those who choose isolation reduce mortality
- Isolation allows life to return to normal.
- Natural immunity and increased immunization with vaccines allow the development of adequate levels of herd immunity and the return of our loved ones to the protected environment
- Most importantly, the isolated VP will certainly no longer die from COVID-19. Because they will be isolated.
The cost is less than the cost of intensive care (2.7.1). Restricting the non-isolated part of society can be maintained to the extent necessary. It is therefore ethically unacceptable for anyone to object to this solution. Safe and infection-free isolation is easy to implement with disciplined, robust execution (4.9). This is not a theoretical epidemiological task, but a simple practical logistics task that should be performed under the guidance of military logistics experts.
The primary reason for elaborating this study in more detail (2.7.2.-2.7.7.) Is that the author tries to prove that the safe isolation of VP is feasible. The technical aspects of the ELSE strategy are nothing more than a strict discipline operation performed under. With proper, accurate planning and inspection, infection should not occur.
If the above-mentioned dangers have an effect at the same time, the number of deaths could be uncontrollably high. So far, the average number of deaths is 10-15 / 10k. The number of people still at risk of death from the virus is in case of R0 = 2.4, HI = 58%, IFR = 0.9% (72/10k-15k) = cc 45/10k, ie 40 thousand people per ten million inhabitantsOn the one hand, in developing countries the vaccination rate is only 5%. On the other hand, there is growing tension between the developing and developed worlds over the non-selfish distribution of vaccines.
For COVID-19, we live in an age of systematic conspiracy theories. Residents of Africa may become particularly susceptible to this, as increasingly fearful fears are embodied on the continent, where the epidemics of the terrible epidemics that are still emerging (eg Ebola) are more frightening than in other parts of the world, due to:
• more sensitive Africans, based on the more valid and acceptable assumptions that
• a genetically engineered virus has been released to them by the Chinese,
• in addition, with the acquisition of valuable (rare earth metals) underground treasures, the Black Continent has been largely colonized and
• proven to be increasingly racist towards indigenous peoples, as evidenced by credible media
• among whom there will be a fear that a flood of enough settlers out of the 1.3 billion Chinese people will be able to fill the “living space”…
There are two more facts that confirm the conspiracy theory for them:
• The number of deaths in China is negligible (EU average: 15,000 / 10 million, China 13 (thirteen!) / 10 million. So far 5,000 deaths / 1.3 billion)
o It is difficult to raise awareness of “Ebola experience for ordinary African natives”, to explain that in China, with the discipline of the Communist Party, strict epidemiological measures can be observed (eg contact tracing, 2 weeks of strict quarantine), in addition to SARS-CoV -1 infection also has a long-standing tradition of restrictions and compliance.
• The vaccine is only shared between developed countries (whites and yellows) with extreme selfishness.
o Vaccination rates are only 5% in Africa and the Third World, compared to 50-80% for whites. This further reinforces the already entrenched racist attitude of blacks towards whites, in addition to the “sino-caucasien-type” collaboration against blacks that has hitherto experienced the devil on the wall in modern history, with a vision of a new world order.
The head of the WHO also drew attention to the above problem: "I have to be raw: the world is on the brink of a moral catastrophe, and the price will be paid by the lives sacrificed in poor countries." {*}
The UN Secretary-General (Guterres) (Reuters, September 2021) {*} has ethically rated the vaccine allocation in the world as the worst. At the company’s annual New York World Congress, he left the following message:“as long as we immunize the world’s welfare societies and throw away unnecessary vaccines in the trash, 90% of Africa has not received a single dose of vaccination” this is a moral indictment to the world, obscenity. We passed the scientific exam, but failed the ethics with an “F” rating”. Guterres plans to get 70% of the world vaccinated.
Guterres also drew attention to a growing geopolitical problem of widening gaps and disparities in U.S. and China economic attitudes, trade, financial and technological rules, and the principles of developing artificial intelligence. According to him, this marks the beginning of another Cold War.
ELSE can supplement the level of herd immunity developed through 60-80% vaccination in the developed world to achieve herd immunity that provides protection at the population level (which can currently be up to 90% stimulated by mutants) while minimizing deaths. In addition, what is perhaps of particular importance is that in underdeveloped regions, where vaccination is only 5% on average with ELSE and COVAX combined, herd immunity could quickly catch up with the developed world and, at the same time, level at a protective level, there is a chance that the virus will be eradicated globally. As you know, the precondition for this is that no patch should remain anywhere in the world that would allow the development of new mutants that break through the flock that has developed. Should this inevitably occur somewhere, a commando with adequate international readiness and equipment would rush to the scene, taking over the management of the measures, with which the local authorities must cooperate unconditionally in all respects, - from the closure of the country, through contact detection, regarding compliance with quarantines - giving them all other assistance.
In the following chapters (Method, Result), we demonstrate how ELSE can help developing countries as well, especially with such a low vaccination rate (5%). Again, the custodian of the eradication of the virus is a coordinated strategy in the world, and especially in these underdeveloped regions, in the framework of an internationally integrated “master plan” based on the main role of ELSE and COVAX.
For the sake of easier comparability, the ELSE-EM also based on all the data and parameters published by the Imperial College COVID-19 Response Team R. Verity{*}, N. Ferguson (Report 9){*} and the Harvard Group M. Lipsitch{*} (default values). Otherwise, the model allows changing all the parameters.
The ELSE Epidemiological Model is based on the separation of the population studied into 2-4 age-groups (AG), the special home quarantine of the different elderly age-groups and the non-restricted working age group. This model makes it possible for the significant portion of all the groups to maintain a normal life and generate herd immunity in a short period.
The epidemiological parameters (ICU burden) of a given elderly age group and the developing herd immunity level, which is controlled by serological survey and compared continuously. By monitoring the processing data, the model schedules the dynamics of the step-by-step entry of a specified number of elderly groups of people at sequenced times from home quarantine into the growing mixing population resulting the further elevation of herd immunity. In addition, our compartmental model reveals the impact of the season force and the mitigation (never mind) suppression parameters to the health care capacity and to the death.
As a consequence of the suggested ELSE program, the overloading of the health care system can be avoided. Consequently, the estimated mortality rate is reduced significantly, and life is rapidly returned to normal way.
The clinical dynamics in our model is based on SIR and SEIR compartmental models, with some relevant extension and modifications. We applied the adapted the SEIRS transmission model{*} according to Kissler (Ref 135).
In order to capture moderate, mild, or asymptomatic infections we considered the following conditions (95.6% of infections), that lead to hospitalization but not critical care (3.08%), and infections that require critical care (1.32%) cases. In this sophisticated and extended SEIRS model, we simulated the disease's progression at a higher resolution. We defined five categories, such as Susceptible (S), Exposed (E), Infectious (I), Recovered (R), Hospitalized (H) and Dead (D). The population can bedivided only into four age groups (AG1–AG4). In the present study for example AG1 = 0–59 years; AG2 = 60–69 years; AG3 = 70–79 years and AG4 = 80+ years. In this model, we used the general transition rates, including average number of contacts per person per time (b), the probability of the transmission to the susceptible from the infectious in a contact (li) and Ni is the fraction of contact occurrences that involve an infectious individual, where i refers to the age groups (AG1–AG4). The rate of hospitalization (ICU, gh,i); recovery (gI,i; patients who recover without the need for hospitalization and gr,i; patients who require hospitalization but survive); or mortality (gm,I; patients who require hospitalization and do not survive) are also included. For the parametrization of the model, only literature and confirmed data were set as the input from references listed here. Each of these variables follows its own trajectory to the outcome, and the sum of these compartments add up to the values predicted by SEIR. Latency periods [t1 = 1/n] were included in the model and they were defined to be as long as 4.6 days. Infectious periods [t2 = 1/g] were also included in the model and they were defined to be as long as 5 days. Between the age groups (AGs) we considered predefined contact matrix (ei,j) between any of the two groups. The element of the contact matrix (ei,j) correspond to the number of contacts per days between the members of the groups.
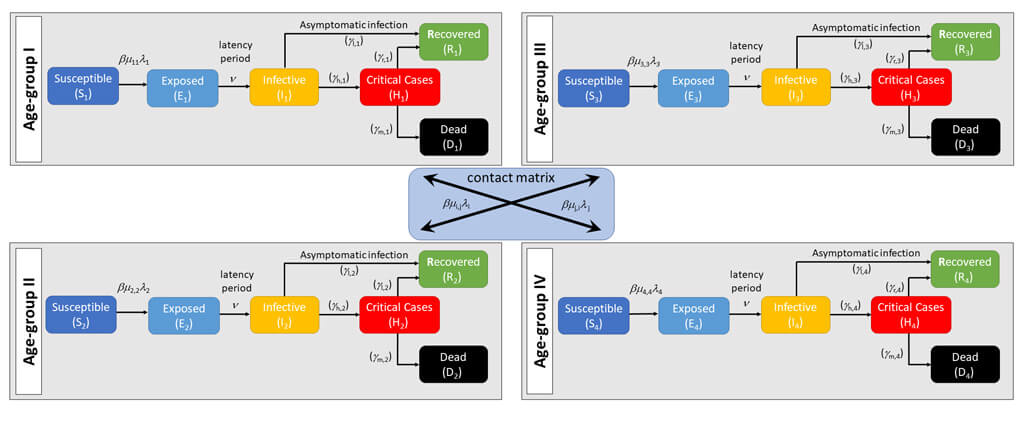
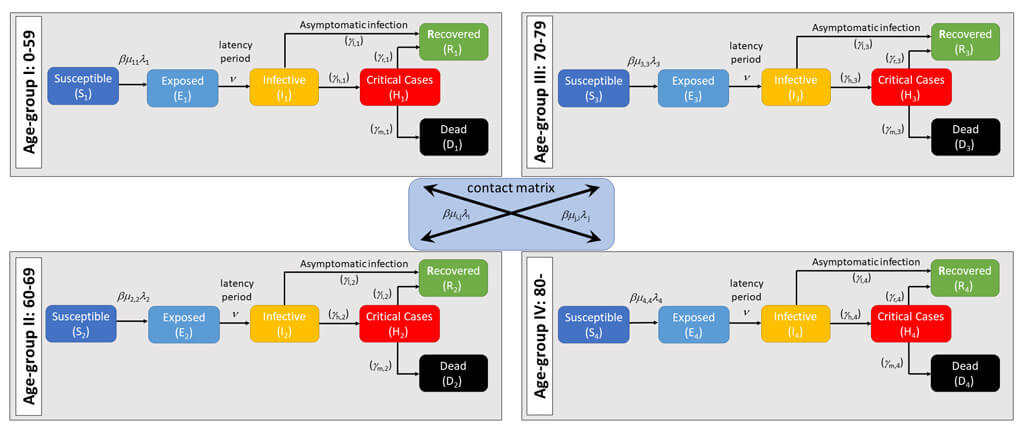
Figure 2.1. The contact matrix of the extended compartment model, including the compartmentalization according to Age Groups (AG-1–AG-4). The age groups can be selected optionally. In the lower table, the default age-groups are presented in the present study. All the subset involves the general dynamic, described by the differential equations.

The definition of the variables, used in the differentia equations and their parametrization used for the current model:

The application can be downloaded: Download
The Explanation of Control Panel (CP) and the Interactive Graphical User Interface (GUI) of the ELSE-EM model. Our proposed dynamic pandemic model is based on 10 differential equations describing the transitions between compartments. We developed our solution using features of Java 1.8 with a highly interactive graphical user interface designed in Swing.
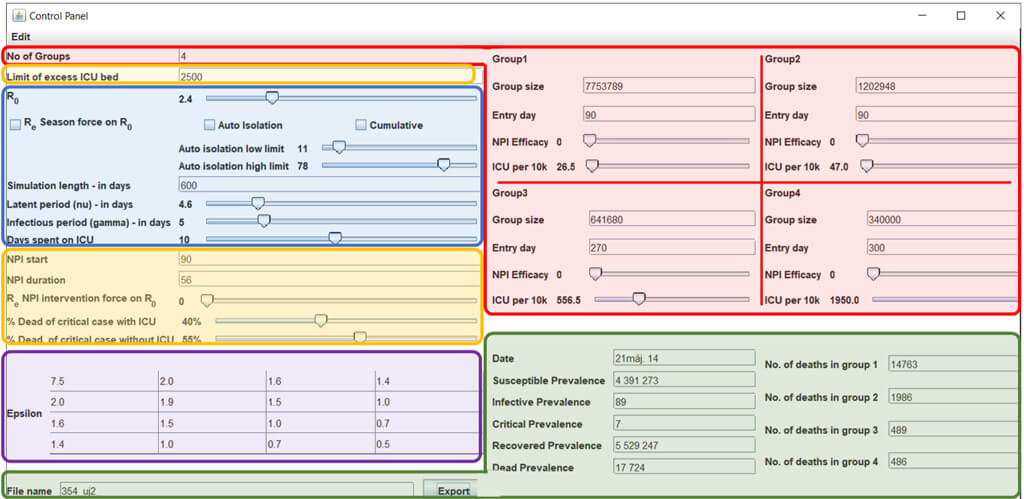
RED: Setting of the population and subpopulations studied.
BLUE: Setting of the pandemic
ORANGE: Setting of the health care system
PURPLE: Interaction of the pandemic with the subpopulations (epsilon).
GREEN: Results. left: Overall results; right: number of deaths for each subpopulation

Figure 2.2. The control panel (CP, upper) and the interactive graphical visualization of the results (GUI, below) of the ELSE program, coded in JAVA (Java 1.8) https://www.raczt.hu/
The Number of Groups means always four in our model by the age stratification, which can be freely varied. For example: Age Group 1: 0-35; Age Group 2: 35-55; Age Group 3: 55-79; Age Group 4: 80+.
Table 2.1. Percentage population in a small central European country of population about 10 million (from https://www.ksh.hu/interaktiv/korfak/orszag.html) by age groups and related ICU/10k values. The death rate of the age groups is based on published data (default numbers . 2.6.2)
| Age group | Age | Size of the subpopulation |
in % | Calculated cases requiring critical care (ICU) |
ICU/10k |
| AG-1 | 0–59 | 7 606 517 | 76.54% | 7 256 | 9.5 |
| AG-2 | 60–69 | 1 176 962 | 11.84% | 18 085 | 154.0 |
| AG-3 | 70–79 | 754 913 | 7.60% | 42 358 | 561.0 |
| AG-4 | 80+ | 400 000 | 4.02% | 78 101 | 1956.0 |
| Sum | 9 938 392 | 100.00% | 145 800 |
It is also possible to set different numbers for the age groups, for example in the developing countries where the “Age-Tree” is significantly different.s shown in Table 2.2. The remarkable result is that the number of VP candidate is less with 20 000 comparing to the developd countries.
Table 2.2. Simulated Percentage population in a developing country of population about 10 million by age groups and the related ICU/10k values.
| Age group | Age | Size of the subpopulation |
in % | Calculated cases requiring critical care (ICU) |
ICU/10k |
| AG-1 | 0–54 | 6 825 406 | 68.7% | 3 927 | 6.0 |
| AG-2 | 55–69 | 1 958 073 | 19.7% | 18 041 | 92.0 |
| AG-3 | 70–84 | 989 132 | 10.0% | 76 442 | 773.0 |
| AG-4 | 85+ | 165 017 | 1.7% | 27 986 | 1696.0 |
| Sum | 9 938 392 | 100.00% | 126 396 |
- The limit of the excess ICU beds means the available Intenzive care unit (ICU) beds for the COVID-19 patients. The default number 2 500. (2.9)
- R0 is defined as the average number of secondary infections generated by a single infected individual in a fully susceptible, well-mixed population. (2.2.1.) In our model the default number is 2.4.
- Re Intervention force on R0 defined – Re: the average number of secondary infections generated by a single infectious individual over an infectious period in a partially immune population. In our case in the CP in the social distance (NPI) duration - as the average number of secondary infections caused by a single infected individual to estimate the reproductive number for an ongoing epidemic, which uses real-life data (from diagnostic testing and/or clinical surveillance) in the population after there is some immunity{*} or interventions have been put in place.{*} Immunity in the population can effectively diminish or end an outbreak by driving Re below 1.{*} „There's one other, unknown factor that will determine how safe it is to loosen the reins: immunity. Every single person who becomes infected and develops immunity makes it harder for the virus to spread If we get 30% or 40% of the population immune, that really starts to change that whole picture, it helps us a lot,”{*} because it would bring R0 down by the appropriate percentage”.{*}
- Herd immunity (HI): the indirect protection from infection conferred to susceptible individuals when a sufficiently large proportion of immune individuals exist in a population Herd immunity threshold: the point at which the proportion of susceptible individuals in a population falls below the threshold needed for transmission. Ongoing outbreak: the effective transmission of a pathogen from an infected individual to susceptible host(s).
- Re Seasonal force on R0: {*}, {*} The decline comparing R0 during the season caused interventional period In our model the maximal wintertime R0 is 2.4 and for the seasonal scenarios in the summertime R0 is reduced to 1.4 (40% decline).
- Simulation length: Days of the simulation. The default value is 600 days
- Latent (nu) and infectious (gamma) period in days, default as 4.6 and 5.0, respectively.: Latency periods [t1 = 1/n] were included in the model and they were defined to be as long as 4,6 days. Infectious periods [t2 = 1/g] were included in the model and they were defined to be as long as 5 days
- Days spent on ICU: The days from 1 (admission) to 20 (discharge) spent on ICU. The default value is 10.
- NPI start: According to the WHO pandemic declaration, we considered the establishment time of sustained transmission on 28 March 2020.
- NPI duration: The days of the interventional force on R0.
- Autoisolation low and high: Assessing intermittent social distancing measures, for which social distancing was turned “on” when the prevalence of infection rose above a threshold and “off” when it fell below a second, lower threshold, with the goal of keeping the number of critical care patients below the given country ICU capacity designated for the Covid -19 cases. In our model we use the 2 500 ICU beds for 10 million inhabitants. (2/10k). In this case the goal can achieve with an “on” threshold of 78/10K and 11/10K “off” threshold.
- Dead of critical case with/without ICU: Fatality rate in percentage with or without intensive care. Our default percentage is 55% without ICU and 40% with ICU. For detailed study see chapter 2.2.2. Infection Fatality Rate (IFR): proportion of deaths attributed to a certain disease among all infected individuals. Case Fatality Rate (CFR): proportion of deaths attributed to a certain disease among all individuals diagnosed with that disease
- Epsilon (e): Social Contact matrix to Estimate Age-specific mixing Transmission pattern for the society. {*}, {*}, {*}, {*}, {*} Our numbers default to the developed countries. For underdeveloped or other specific country can use the latter study from the 152 countries results using contact surveys and demographic data.
- Group size: The population of the specified groups(AG1-AG4) from the total inhabitants. The group size can very like the example in the ICU per 10k.
- Start day: The day of entry of a specified Group from home quarantine into the growing mixing population. The epidemiological parameters (ICU burden) of a given elderly age group and the developing herd immunity level, controlled by serological survey will be continuously compared. By monitoring the processing data, the model schedules the dynamics of the step-by-step entry of a specified number of elderly groups of people at sequenced times from home quarantine in to the growing mixing population resulting the further elevation of herd immunity.
- NPI Efficacy value of the Groups: Non-Pharmaceutical interventions, means the protection by cloths, gloves, and masks. (li) Infectious potency by groups, the infectious potency of the infectious person, depending on the protective gear it is 1.0, when the transmission impossible it is 0.0, without any protection (3.6.)
- ICU per 10k: ThenumberICU beds burden per 10k population in the given Group by the table (2.6.2.2.) adapted by the Report-9 of the Imperial College.{*} In this table the „% hospitalised cases requiring critical care” column indicate the designated ICU beds burden per 10k population.
- The date, susceptible, infective, dead prevalencesare cases at a given time indicated by the position of the cursor from the GUI. The critical cases reach a plateau by the limit of excess ICU beds. The Recovered cases indicate the actuel Herd Immunity level at the same time.
ELSE VP protocol is developed, in order to protect the vulnerable population, because years long quarantine period cannot be tolerated between indoors. The most effective and safe version to isolate the in Cruisers, Resorts and Hotels. (VPCRH 2.7.1.3). The ELSE VP strategy allows, on the one hand, the working age group to start working, live a full life within a month after the start of the intervention, on the other hand, it allows the economy to recover, and finally the vulnerable members of the whole population will almost completely escape from death. These could be achieved without overloading the health system. With the generation of herd immunity (HI), the development of the safe vaccine will be possible, duing this time. Finally, the VP will be released to the safe, herd immunity protected environment and the scenario is complete.
The isolation of VP will last for a couple of months until the HI reach the appropriate level of protection. To assess the number of VP it is necessary to estimate the infection fatality rate (IFR). Significant number of studies researched and exhbited large variety of numbers. For example, from the Imperial College COVID-19 Response Team (Report-9, the default parameter source of this article was taken from this report). In the original Chinese data estimated the IFR to be the average between 0.2% and 1.6% in all age-groups, while in the oldest age group (≥80 years), it rates range from 8% to 36%.{*} In March many data were compiled by Imperial College confirming the data has been accumulated since then. The analysis of LSTH and UCLA consider plausible range of R0 values spanning 1.5–4.0, with 4.0 representing a plausible maximum in the absence of any behavioral changes or containment efforts, and 1.5 reflecting a plausible lower bound, given containment measures may already be in place at the time of introduction.{*} Recent study from Iceland estimates the IFR of 0.3%.{*} The median IFR was 0.24% inferred from seroprevalence data.{*}
The aggregated best estimate, taking account of historical experience, trends in the data, increased number of infections in the population at largest, and potential impact of misclassification of deaths gives a presumed estimate for the COVID-19 IFR somewhere between 0.1% and 0.41%.{*} Case Fatality rates vary significantly, between countries{*} in this CEBM Oxford study.
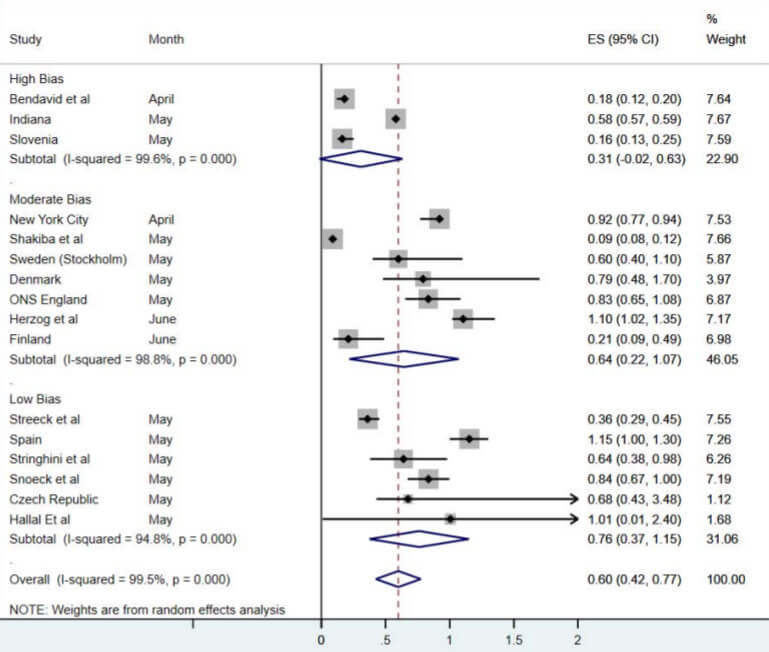
Table 2.2.1. Meta-analysis of IFRs of COVID-19 from serosurveys by risk of bias. Taken from ref. {*}
In this systematic review and meta-analys the aggregated estimate across all 24 studies indicated an IFR of 0.68% (95% CI 0.53-0.82%), or 68 deaths per 10,000 infections. Heterogeneity was extremely high, with the overall I2 exceeding 99% (p<0.0001). However, due to very high heterogeneity in the meta-analysis, it is difficult to know if this represents the true point estimate. It is likely that, due to age and perhaps underlying comorbidities in the population, different places will experience different IFRs due to the disease. The R0 estimated in a meta-analysis 3,15{*} and in an other study varied from 2.2 to 6.47 (2.2 Riou és Althaus, 2,2 Li et al., 2,6 Imai et al., 2,7 Wu et al., 3,8 Read et al., 4.5 Liu et al., 4.08 Cao et al.,4.7 Sanche et al., 6,3 Sanche et al., 6,47 ){*} Recent study of the New York City cases revealed IFR of 0.97%.{*}.Tang et al.
The author concludes that the optimal methodology to approach the real circumstances if the default number of IFR is 0.9% for the situation without ICU, (slider in the CP is positioned at the 55% value) while the mortality rate reduced by 40% for those who receive ICU therapy (IFR = 0.6). Of course, the desired value can be freely set in the Control Panel via the slider. (From zero to 100% i.e. up to 1.6% IFR by these parameters of the CP). See next section 2.2.2.)
In the estimation of IFR, it should be evidently reasonable to take into account as an important influencing factor, the presence or absence (admission rate) of ICU, whether the death occurred without ICU therapy or with the use of ICU therapy. In this regard, the studies certify or carry out some sort of laissez-faire elegancy.
This section is essential in the ligth of the parametrization of the epidemic model. We should estimate the number of people, who requires intensive care after the infection (ICU/10k) and the fatality rate with and without the intensive care.
As an unequivocal example, on the Diamond Princess{*} where not a single ICU was present, the estimated IFR were 1,3% for all ages and 6,4% over 70 years and CFR 2,6% and 13%{*} respectively, among the senior passengers.
In the overwhelmed health care difficult to evaluate the access rate to ICU treatment. In Chinese studies 29% of the ICU patients who died, did not receive mechanical ventilation, and where systems experienced a surge of critically ill patients, up to 53.2% of patients who required ICU care were unable to receive it because of resource constraints. In New York, 262 deaths occurred in hospital wards and outside the ICU, compared to 291 deaths in the ICU{*}
At three hospitals in Atlanta, US the overall mortality to date in a critically ill cohort is 30.9% (67/217) and 60.4% (131/217) patients have survived to hospital discharge. Mortality was significantly associated with older age, lower body mass index, chronic renal disease and receipt of mechanical ventilation. Despite previous worldwide multiple reports of mortality rates exceeding 50% among critically ill adults, particularly among those requiring mechanical ventilation, early experience in Georgia state indicates that many patients survive their critical illness.{*}
The most convincing data from 24 studies including 10,150 patients demonstrate an ICU mortality rate (95%CI) in those with a completed ICU stay of 41.6% (34.0%–49.7%). The high degree of heterogeneity (I2 = 93.2%) in the meta‐analysis suggests that survival rates between studies are highly variable. This mortality is broadly consistent across the globe. As the pandemic has progressed, the reported mortality rates have reduced from above 50% in March 2020 to close to 40% at the end of May 2020. This in‐ICU mortality from COVID‐19 is higher than usually seen in ICUs for other viral pneumonias. Further, the overall mortality from completed episodes of ICU differs considerably from the crude mortality rates in some early reports.{*}
However, none of the studies provides information about the influence of the presence or absence of ICU on IFR, except of course the Diamond Princess cases. However, there are several limitations to conclude relevant information for the real-life circumstances, for example the average year of 58.
The only study affords the possibility to estimate the effect influence of the presence or absence of ICU on mortality can derive from the Italian experience.
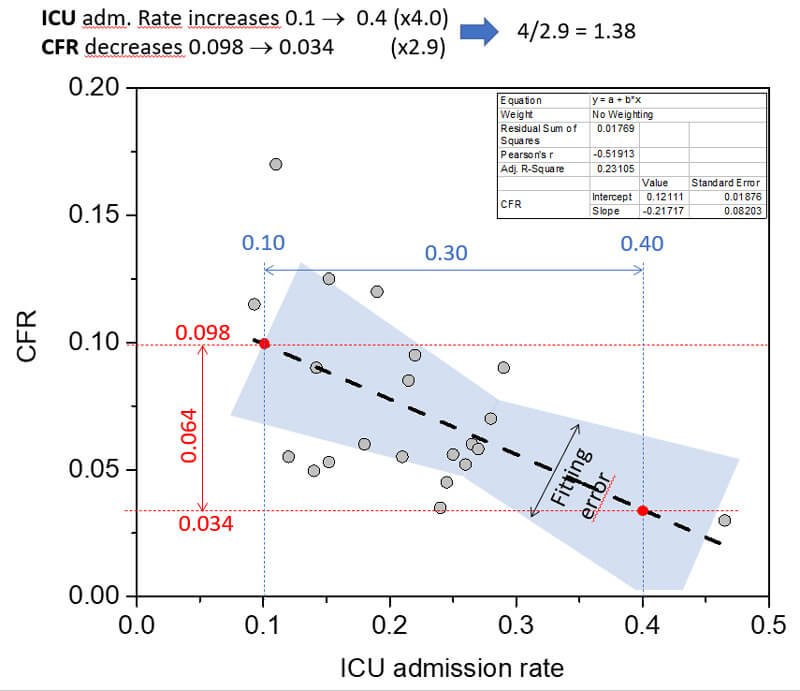
Figure 2.2.2. Data from 20 regions were collected; the average interregional case fatality rate (CFR) was 7.5%, range 3.1–16.7%, and the average ICU admission rate was 21.4%, range 9.4–45.9%. A statistically significant negative correlation was observed between the CFR and ICU admission rate (Pearson’s r −0.53, p value 0.014) and R2 was 0.24, suggesting an association between mortality and the absence of treatment in ICU. Modified from Immovilli et al.{*}
Based on the most convincing article the %Dead of critical case with ICU was set at 40% as default in the CP. Based on the Italian study, when ICU is overwhelmed, the % Dead of critical case without ICU situation was estimated 1.38 times higher than the ICU, namely non-ICU is 40%*1.38 = 55%. We consider the IFR of 0,9% of the Imperial Collage study, as the default number of % Dead of critical case without ICU.
- The IFR is 0.6% when the %Dead of critical care with ICU is set at 40%, (default)
- The IFR is 0.9% when the %Dead of critical care without ICU is set at 55%, (default)
- The IFR is 1.6% when the %Dead of critical care with ICU is set at 100%. (There is a possibility to set the slider for any kind of different)
Further caution should be maintained to draw real conclusions from the interpreted statistics. The Public Health England’s definition of the daily death figures means that everyone who has ever had COVID at any time must die with COVID too.{*} The true extent of the coronavirus disease 2019 (COVID-19) epidemic in the US is unknown. The 3.4 million confirmed cases reported (as of July 15, 2020) likely represent only a fraction of all the infections that have occurred in the US thus far.{*} In a study coordinated by the CDC revealed that it is difficult to imagine a successful next phase of the epidemic response that does not address the vast numbers of undetected infections still at large in the community.{*} Epidemiologists have expected that only about 10 percent of the cases will be reported.{*} Estimated cumulative cases and deaths by MIT team data from 84 countries are 10.5 and 1.47 times official reports, yielding an infection fatality rate (IFR) of 0.65%, with wide variation across nations.{*} The director of the CDC announced, that the CDC conducted seroprevalence estimates suggest that >10 times more SARS-CoV-2 infections occurred than the number of reported cases by the underlying scientific report.{*}
Moreover, very recently, the WHO announced to attendees from member governments that about 10 percent of the global population may have been infected by SARS-CoV-2 virus. This estimation on October suggests that >23 times more infections occurred than the confirmed cases.{*}
According to the abovementioned studies, the currently reported 100 million cases (end Jan 2021) could be more than 1 billion or 2 billion cases of SARS-CoV-2 infection. Based on this number from the 2 million death cases the calculated IFR: 0.20% and 0.10% respectively.
Furthermore, data from more than 30 countries the estimated excess deaths are 25 % more, than would normally be predicted.{*}
The well-founded causativeness between preexisting chronic diseases and COVID-19 related to mortality has not been determined yet exactly for several reasons,
- the limited number of comprehensive, conclusive studies, more relevant studies with more careful design, more rigorous execution, and larger sample size with less publication and data collection bias.
- the studies often faile to describe all relevant characteristics of individual patients and therefore difficult to adjust for potentially confounding factors such as age, gender, ethnicity (profound studies of the outbreak from China) and use of treatments.
- the pronounced heterogeneity among studies in the patient’s size, design, lengths of follow-up, furthermore the definitions of severity, diagnose and biomarkers of the diseases. For example, from the WHO Cardiovascular diseases group, the definition lacks the Cardiac Injury instead “coronary heart disease (heart attack)” is. The word congestive{*} is missing, only ‘heart failure’ is included.{*} The exact definition of cardiac injury is not included in any of the studies.{*}
- MINORS (instrument designed to assess the methodological quality of non-randomized surgical studies, whether comparative or non-comparative){*} rating scale: (1) A clearly stated aim; (2) Inclusion of consecutive patients; (3) Prospective collection of data; (4) Endpoints appropriate to the aim of the study; (5) Unbiased assessment of the study endpoint; (6)Follow-up period appropriate to the aim of the study; (7) Loss to follow up less than 5%; (8) Prospective calculation of the study size; (9) Appropriate selection of control group; (10) Synchronization of control group; (11) Baseline comparable between groups; (12) Appropriately statistical analysis. The global ideal score being 24 for comparative studies.
- TRIPOD (transparent reporting of a multivariable prediction model for individual prognosis or diagnosis) also a guideline for studies.
The usually applied Cochrane’s Q test is capable to inform only the presesence or absence but not the extent of heterogeneity, that is very important in the rapidly evolving similarly heterogeneous studies of the COVID-19 concerning the prediction factors (OR: Odds Ratio; HR: Hazard Ratio) of critical and/or death cases. Instead of this fixed-effects model, random-effects models preferred to use supposing that there may be different underlying true effects estimated in each investigation that are distributed about an overall mean. The confidence intervals (CIs) around the mean include both within-study and between-study components of variance and likewise uncertainty. Summary or bottom line effects provide an estimation of the average treatment effect, and the CI depicts the uncertainty around this estimate.{*}The inconsistency (I²) index refer to the degree or dispersion while the T2 and T or Tau quantify the amount of heterogeneity.{*} Together with the point estimate and CIs, these elements express more practical, real-world implications of the observed heterogeneity.
The greater the heterogeneity (variability) in effect sizes of the underlying studies, the greater the un-weighting and this can reach a point when the random effects meta-analysis result becomes simply the un-weighted average effect size across the studies. At the other extreme, when all effect sizes are similar (or variability does not exceed sampling error), and the random effects meta-analysis defaults to simply a fixed effect meta-analysis (only inverse variance weighting).{*}Therefore, the proper choice of interpretation and assesement of studies heterogeneity by the fixed or the random-effects meta-analysises have mounting importance, providing sufficient data to help defining the selection criteria of the vulnerable patients.
Creative skills should be adapted comparing the reconciled time traditional meta-analysis to properly distinguish, evaluate and retrieve relevant information from amongst the rapidly evolving new ones associated with COVID-19.
The selected articles helping to set up the selection criteria. (2.5.)
The author is aware that this part of feasibility of the VP protocol is one of the critical tasks, therefore he would like to reiterate that the the selection criteria of the patients is a representative demonstration with suggested guidelines of the solution proposal. The final criteria should be finalized by WHO, CDC, Tessy and the countries national health authorities.
Even though the large number of elderlies, who are a wide range comorbid sufferers – of which the majority not related to COVID-19 - a rational complex professionally approach based on the relevant scientific report, systemic reviews and metaanalysis, could defines and confines the number of patients who potentially really could be exposed to serious risks of Covid -19.
The final step of selection belongs to the GPs, who by their professionally and personally knowledge about the potential VPs are able to conclude to the final decision, the objectivity of which is ensured by the associated professional scores. In this way, the resulted limited number of VPallows them to isolate with high military security and multiple buffers.
The determination of precise selection parameters focuses on the more severe disease that leads to intensive care unit admission, ventilation, especially death from underlying health, which increases the risk of serious human disease with COVID-19, keeping in mind, the basic principles of the pathomechanism.
The reported numbers, tables, and ideas are only the proposal of the author. The concluded suggestions, recommendations, schemes, examples and illustrations, inspiration is for the solution of the current situation. In the future, more accurate and precise selection criteria should be based on broader up-to-date data adapted to local morbidity and mortality conditions.
We can compile an even more balanced standard for defining selection criteria if the basic pathogenesis is kept in mind as a guiding principle. This is particularly important for closing the selection procedure at GPs who are personally familiar with patients. The GPs can more effectively identify those with severe preexisting condition leading to death. In order to gain enough in-depth knowledge of the COVID-19 pathomechanism further training is needed for them before the ELSE starts.
According to this guiding principle, the virus that invades the upper and then lower respiratory tract impede the uptake of oxygen and obstructs pulmonary blood perfusion. The gradually decreasing compensation of this strain by the heart with its preexisting and/or reduced reserve capacity due to underlying disease(s), leading to a cascade process leading to death due to the severe acute respiratory syndrome as main symptom and then the consecutive progressive collapse of the kidney and other organ functions{*}
Chronic conditions cause dysregulation of major physiological systems, including the hypothalamic–pituitary–adrenal axis, the sympathetic nervous system, and the immune system. The chronic nature of such preexisting conditions imposes a growing allostatic load, induces the ‘‘wear and tear’’ on the body’s regulatory systems, leading to the accumulation of pro-inflammatory cytokines, which affects the immune system, resulting more susceptibility to severe complications of SARS-CoV-2 and death. An in-depth, detailed analysis of the immunological,{*}, {*} functional,{*} genetic,{*} and other{*} aspects of the pathomechanism are evaluated in several excellent articles.
The final closure of the path leading to the death is cardiac arrest, as the rest of the body works as long as the ever-deteriorating capacity for as long as the heart. Moreover, this is where the problem with statistics continuing with the raw data recording, which must be taken into account when setting professional standards. That is a great difference in how deaths are attributed to SARS-CoV-2: dying with the disease (association) is not the same as dying from the disease (causation).{*} The primary parameter, by the professional rules is the maintenance of vital especially the cardiac function, which is monitored by ICU staff.{*} With cardiac arrest, heart failure usually will also be identified as the primary cause of death. Although this decrease in cardiac capacity developed here intensively, similar to the decrease in capacity of other organs one impairing the function of the other and vice versa. Statistics therefore tend to blur and overlapped the preexisting cardiovascular disease - if it was at all - and the fatal heart failure that developed at the ICU. This underestimates the importance of other underlying diseases, even though they caused cardiac arrest as an end result. Therefore, on the one hand, it is correct, as the CDC explains it more clearly in defining the precondition of the heart: "serious heart conditions, such as heart failure, coronary artery disease, or cardiomyopathies." On the other hand, with this in mind, other organ diseases that are thus underestimated should be treated at their proper value and carefully considered.
Related to this is the different severity classification of hypertension. The initial and especially Chinese data attach pronounced importance to it. And here again, if the patient has not previously been shown to have significant impaired cardiac function, but hypertension does, the intensive care physician logically associates hypertension with cardiac arrest, although it is easily possible that hypertension is a starting kidney or metabolic syndrome was a more manifest side effect. In general, of course there is an obvious association between hypertension and cardiac arrest.
In line with the CDC, people of any age with certain underlying diseases have an increased risk of severe illness due to COVID-19.{*}, {*}, {*} The CDC definedsevere illness as hospitalization, admission to the ICU, intubation or mechanical ventilation, or death.{*}
Following CDC if the evidence for COVID-19 is associated with severe disease meets any of the following criteria:{*}
Strongest and most consistent evidence: Defined as consistent evidence from multiple small studies or a strong association from a large study,
- Mixed evidence: Defined as multiple studies that reached different conclusions about risk associated with a condition, or
- Limited evidence: Defined as consistent evidence from a small number of studies.
CDC: Patients of any age with the following disease have an increased risk of serious illness due to COVID-19:
- Cancer
- Chronic kidney disease
- COPD (chronic obstructive pulmonary disease)>
- Immunocompromised state (weakened immune system) from solid organ transplant
- Obesity (body mass index [BMI] of 30 or higher)
- Serious heart conditions, such as heart failure, coronary artery disease, or cardiomyopathies
- Sickle cell disease
- Type 2 diabetes mellitus
People with the following conditions might be at an increased risk for severe illness from COVID-19:
- Asthma (moderate-to-severe)
- Cerebrovascular disease (affects blood vessels and blood supply to the brain)
- Cystic fibrosis
- Hypertension or high blood pressure
- Immunocompromised state (weakened immune system) from blood or bone marrow transplant, immune deficiencies, HIV, use of corticosteroids, or use of other immune weakening medicines
- Neurologic conditions, such as dementia
- Liver disease
- Pregnancy
- Pulmonary fibrosis (having damaged or scarred lung tissues)
- Smoking
- Thalassemia (a type of blood disorder)
- Type 1 diabetes mellitus
(The summary of the related studies of this section is in Table. 2.4.3.)
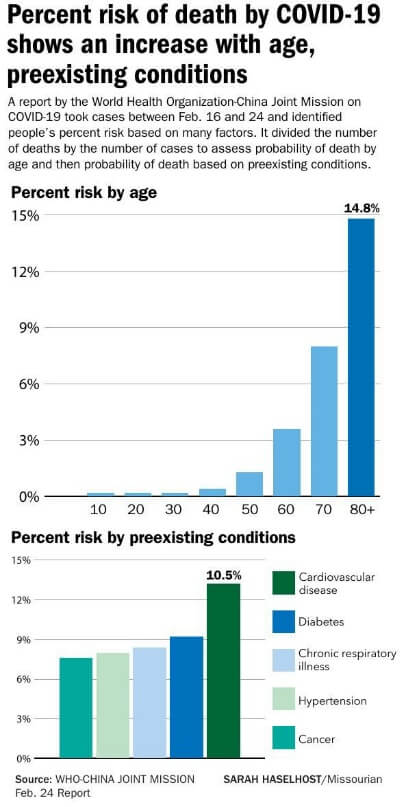
Figure 2.4.3. WHO Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) 16-24 February (2020){*}
The selection criteria based on the preexisting condition; comorbidities projected from the data of WHO. Mortality increases with age, with the highest mortality among people over 80 years of age. Patients with comorbid conditions had much higher rates: 13.2% for those with cardiovascular disease, 9.2% for diabetes, 8.4% for hypertension, 8.0% for chronic respiratory disease, and 7.6% for cancer. While patients who reported no comorbid conditions had a CFR of 1.4%.
The Imperial College in Report-9 used this WHO’s data. Both published data based on the Chinese statistics and published information.
Other data, which have accumulated since then, show a similar pattern.{*}, {*}
According to data reported to the European Epidemiological Surveillance System (TESSy, the underlying diseases of patients who died of COVID-19 by 22 April were also similar. (based on data from 5,378 patients){*}
Estimated case fatality among patients who received ICU care was similar in CDC report and the COVID-19 Response Team stated that all adults, regardless of underlying conditions or age, are at risk for serious illness from COVID-19.{*} Furthermore, the CDC COVID-19 Response Team also reported from among 7 162 patients, by underlying health condition, and risk factor for severe outcome in US February 12–March 28, 2020.
The WHO reported relatively few cases of infants confirmed to have COVID-19. Those who are infected have experienced mild illness. Robust evidence associating underlying conditions with severe illness in children is still lacking. Among 345 children with laboratory-confirmed COVID-19 and complete information about underlying conditions, 23% had an underlying condition, with chronic lung disease (including asthma), cardiovascular disease, and immunosuppression most commonly reported. Recently, case reports and small series have described a presentation of acute illness accompanied by a hyperinflammatory syndrome, leading to multiorgan failure and shock. According to WHO only initial hypotheses are that this syndrome may be related to COVID-19 based on initial laboratory testing showing positive serology in a majority of patients.{*}
Other study revealed similar conclusion with children.{*} One possible explanation could be the presence of pre-existing humoral immunity in uninfected and unexposed humans to the new coronavirus. SARS-CoV-2 S-reactive antibodies were detectable in SARS-CoV-2-uninfected individuals and were particularly prevalent in children and adolescents.{*} COVID-19 incidence among adolescents aged 12–17 years was approximately twice that in children aged 5–11 years. Underlying conditions were more common among school-aged children with severe outcomes related to COVID-19.{*}
Different studies claim that the reason of this phenomenon is based on the robust T-cell activity of the youngest generation or the children’s T cells are untrained, so they might have a greater capacity to respond to new viruses. Alternatively, children might have a strong innate immune response from birth, although that raises the question of why it is not seen with other viruses that can cause severe disease in children. On the other hand, it could be thanks to the protection of antibodies to seasonal common-cold coronaviruses, which run rampant in children. Kids might receive a smaller dose when exposed to SARS-CoV-2, because their noses contain fewer of the ACE2 receptors that the virus uses to gain access.{*}
Swiss study reported 5,039 confirmed cases by seroprevalence. Of the 286 reported deaths caused by SARS-CoV-2, the youngest person to die was 31 years old. They estimated similar IFRs (range 0.00032-0.0016%), in younger than 50 years, in 50-64 years 0.14%, in 65 years and older 5.6%, while a population wide IFR of 0.64%.{*}
Iceland study with stratified by age, the IFR was substantially lower in those 70 years old or younger (0.1%; 95% CI, 0.0 to 0.3) than in those over 70 years of age (4.4%; 95% CI, 1.9 to 8.4).{*}
In a JAMA study mortality rates for those in the 18-to-65 and older-than-65 age groups who did not receive mechanical ventilation were 1.98% and 26.6%, respectively. There were no deaths in the younger-than-18 age group.{*}
Table. 2.4.3. Percentages of the death and preexisting conditions
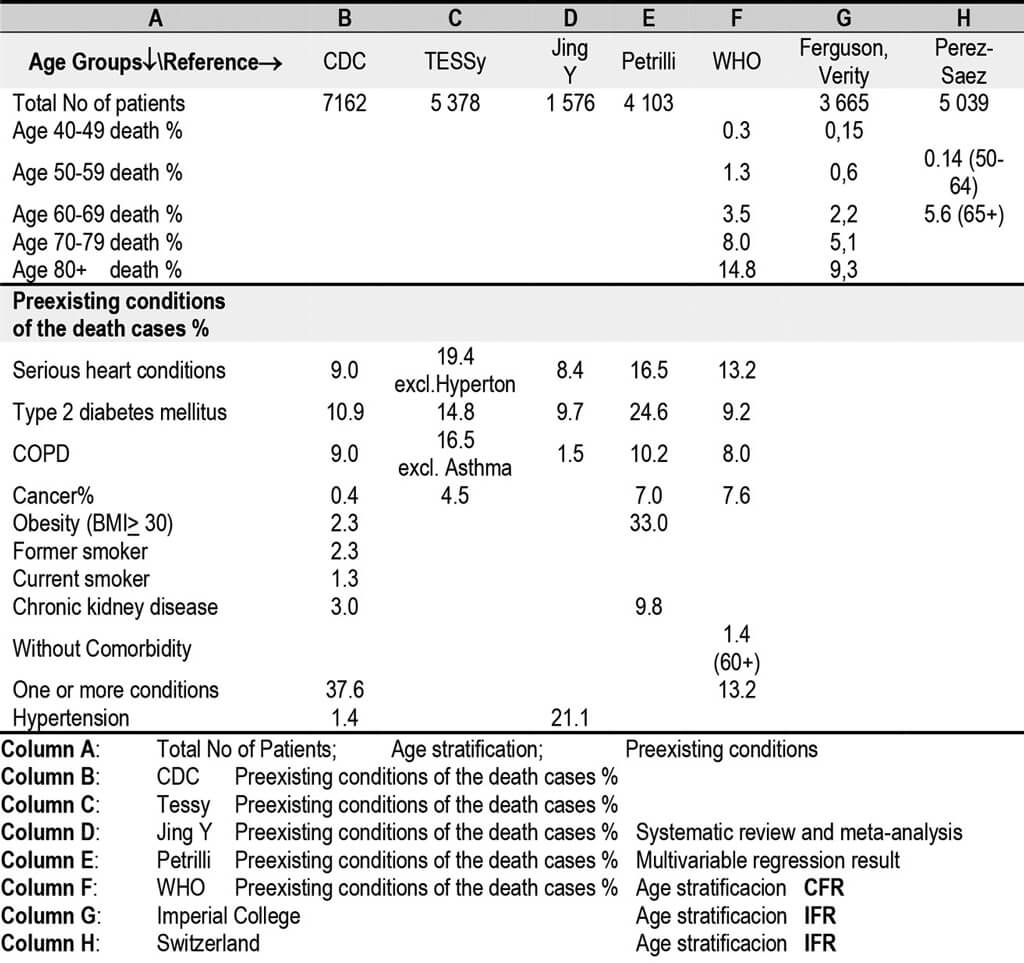
(The summary of the related articles is in Table. 2.4.4.)
In agreement with CDC, one of the most convincing results of the available meta-analysises found is that of Zheng, Z et al. systematic review of the risk factors of critical & mortal COVID-19 cases. They took thoroughly the minor evaluation into account and applied the fixed and random effect model convincingly and they conducted the necessary sensitivity and soubgroup analysis, too, inculuding 13 studies and 3 027 patients. They used the I2 statistics to assess the magnitude of heterogeneity: 25%, 50%, and 75% represented low, moderate, and high degrees of heterogeneity, respectively. The chosen of the proper effect model was based on the analysis results: the fixed effect model was used if I2 ≤ 50% and the random effect model was used if I2>50%. If there was statistical heterogeneity among the results, a further sensitivity analysis was conducted to determine the source of heterogeneity. After the significant clinical heterogeneity was excluded, the randomized effects model was used for meta-analysis. P < 0.05 was considered as statistical significance. The proportion of underlying diseases such as diabetes, cardiovascular disease, and respiratory disease were statistically significantly higher in critical/mortal patients compared to the non-critical patients.the heterogeneity test results were calculated as I2=45%, 37% and 50%. Thus, the fixed-effect model was used for further analyses.
- Diabetes: OR=3.68, 95% CI (2.68, 5.03), P < 0.00001; Heterogeneity: Chi2=18,12 df=10 I2=45%,
- Cardiovascular disease: OR=5.19, 95% CI (3.25, 8.29), P < 0.00001; I2=37%,
- Respiratory disease: OR=5.15, 95% CI (2.51, 10.57), P < 0.00001). I2=50%,
- Hypertension: OR=<2.72, 95% CI (1.60,4.64), P=0.0002; the heterogeneity test showed that I2=72%. Given that the severity of illness and severity of epidemic might contribute to the heterogeneity, we classified the studies into two subgroups according to whether the study site was located in Wuhan. However, heterogeneity still exists. So, the random effect model was used. The result indicated a higher proportion of hypertension in critical/mortal.
- Malignancy, the fixed-effect model (I2=0) meta-analysis showed that the proportion of malignancy was higher in critical/death group yet without statistical significance [OR=1.60, 95% CI (0.81, 3.18), P=0.18]
- Age over 65 years old: OR =6.06, 95% CI (3.98, 9.22), P < 0.00001;
Smoking and male, older than 65, and smoking were risk factors for disease progression in patients with COVID-19 (male: OR=1.76, 95% CI (1.41, 2.18), P < 0.00001; current smoking: OR =2.51, 95% CI(1.39, 3.32), P=0.0006). Smoking patients might face a greater risk of developing into the critical or mortal condition and the comorbidities such as hypertension, diabetes, cardiovascular disease, and respiratory diseases could also greatly affect the prognosis of the COVID-19.
Remarkable the systematic review and meta-analysis Jing Y et al. They assessed the prevalence of comorbidities in the COVID-19 patients and found that underlying disease, including hypertension, respiratory system disease and cardiovascular disease, may be risk factors for severe patients compared with non-severe patients. The study included 1 576 infected patients, however among them one included 1 099 (Guan) another one included 9 patients (Huang) represented by the corresponding weights. (1-93%). The different lengths of follow-up may miss the events leading to heterogeneity. Because only a few studies compared the comorbidities of severe and non-severe patients, they did not conduct sensitivity and subgroup analysis. Furthermore, indpendently of the I2 value (0-62%) they used random effect model.
Ssentongo, P., et al., study is a systematic review and meta-analys is across Europe, Asia and North America, with a admirable sample size (N=61 455) and number of studies (n=19), however among them the study fom Feng et al. represented 44 000 patients alone. They used random effect modell independently of I2 value (0-87%) although they applied Egger’s test and funnel plot. Maybe it does not happen in this particular, - otherwise excellent - study, but the overwhelming large study size effect (N=44 000 vs 61 455) and the consequent use of the random effect model can result the redistribution of weights in one direction from larger to smaller studies and the heterogeneity increases until eventually all studies have equal weight, and no more redistribution is possible.{*}
The findings otherwise suggest that patients with preexisting chronic conditions had a higher risk of death from COVID-19 in the following cases:
- With any (!) cardiovascular disease was 2.35 times (RR ranged 0,72-6,0) (95% CI: 1.44-3.84), implying a 2-fold increase in mortality. Between-study variation was moderate (I2 = 65, p =0,01 Egger’s test p=0.83 and funnel plot indicated no publication bias).
- With coronary heart disease were 2.4 times (RR= 2.40, 95%CI=1.71-3.37, n=5, I2 = 0,0%, (Fenget al. is not in the group.) p= 0,79 Egger’s test p=0.45 and funnel plot indicated no publication bias).
- With hypertension were 1,89 times (RR=1.89, 95%CI= 1.58-2.27, n=9 I2 =0,0%, , p=0,61 Egger’s test p=0.87 and funnel plot indicated no publication bias). Wiith cancer were 1,93 times (RR=1.93 95%CI 1.15-3.24, n=4 I2 =22%, p =0,01).
- With congestive heart failure were 2.5 times (RR=2.66, 95%CI 1.58-4.48, n=3 I2 =0%, p=0,82). With COPD were also at a significantly higher 1.76 times (95% CI: 0.92-3.36), (I2 = 73, p =0,01 Egger’s test p=0.43 and funnel plot indicated no publication bias)
- With chronic kidney diseas, the risk of mortality from COVID-19 in patients showed no significant association (RR: 2.36 95% CI: 0.97-5.77). Between-study heterogeneity was medium (I2 = 63%, p=0.04).
- With chronic liver disease, the risk of mortality from COVID-19 in patients found no association. RR: 1.57 95% CI: 0.70-3.50. Between-study heterogeneity was low (I2 = 0%, p=0.32).
- With preexisting type 2 diabetes the risk of mortality from COVID-19 in patients were not significant (RR: 1.37, 95% CI: 0.85-2.20). Between-study heterogeneity was high (I2 = 87%, p =0,01)
They did not find studies reporting association asthma and COVID-19 risk of mortality.
Cohort study analysed by Cox-regression to generate hazard ratios: age and sex adjusted, and multiply adjusted for co-variates selected prospectively +based on clinical interest and prior findings. Determinants of COVID-19 disease severity in patients with cancer. Age older than 65 years and treatment with immune checkpoint, whereas receipt of chemotherapy and major surgery were not. Tracking patient responses over time sheds light on this issue and has implications for efforts to predict disease severity.
Although there is a knowledge gap, as to which aspects of cancer and its treatment confer risk of severe COVID-19.{*}
In the Cohort study of Williamson, E., et al., (LSHT London, CTM Oxford) the Hazard Ratio associated with COVID-19-related hospital death in the linked electronic health records of 17 million adult NHS patients show in Table 2.4.4.
Similar study by the same and other groups LSHT, CTM, UCL, NHS, Imp. Coll. derive and validate a risk prediction algorithm to mortality outcomes from covid-19 in adults. Adjusted hazard ratio (95% CI) of death from covid-19 in men in derivation cohort, adjusted for variables shown, deprivation, and fractional polynomial terms for body mass index (BMI) and age are shown in Fig. 2.4.4.{*}
A retrospective cohort study by Chen, R et al. of 1,590 hospitalized patients with COVID-19 throughout China displays independent factors for the fatal outcome.
In the study of Petrilli, C.M. et al. demonstrate the factors associated with critical illness among 4,103 patients with COVID-19 disease in New York City in a multivariable regression result.
In Wang, L. et al study high proportion of severe to critical cases and high fatality rate were observed in 331 consecutive cases over 60 years old.
Lippi et al results demonstrated an five fold increased risk of COPD associated with severe COVID-19 infection.{*}
Fadin, G.P., et al. in their six of the meta-analysed studies on Chinese patients (n = 1687). The pooled rate ratio of diabetes among patients with adverse disease course as compared to those the more favourable course was 2.26 Based on these data, they conclude that diabetes may not increase the risk of SARS-CoV-2 infection but can worsen the outcome of this new coronavirus disease.{*}
Swiss study with 5,039 confirmed cases by seroprevalence. Of the 286 reported deaths caused by SARS-CoV-2, the youngest person to die was 31 years old. They estimated similar IFRs (range 0.00032-0.0016%), in younger than 50 years, in 50-64 years 0.14%, in 65 years and older 5.6%, while a population wide IFR of 0.64%. Iceland study with stratified by age, the IFR was substantially lower in those 70 years old or younger (0.1%; 95% CI, 0.0 to 0.3) than in those over 70 years of age (4.4%; 95% CI, 1.9 to 8.4).{*}
In a JAMA study mortality rates for those in the 18-to-65 and older-than-65 age groups who did not receive mechanical ventilation were 1.98% and 26.6%, respectively. There were no deaths in the younger-than-18 age group.{*}
In case series of 4 young male patients with severe COVID-19, rare putative loss-of-function variants of X-chromosomal TLR7 were identified that were associated with impaired type I and II IFN responses.{*} A recent genomics study reveals excess mutations involved in the regulation in the type I and III IFN pathway that may determine the clinical course of the infection.{*} The same group in a large immunological study of COVID-19 patients, identified individuals with high titers of neutralizing autoantibodies to type I interferons (IFN-α2 and IFN-ω) in about 10% (2,6% women, 12,5% men) of patients with severe COVID-19 pneumonia. These autoantibodies were not found either in infected people who were asymptomatic or had milder phenotype or in healthy individuals. Together, these studies identify a means by which individuals at highest risk of life-threatening COVID-19 can be identified. Screening patients - that takes two days - for autoantibodies against interferons is a new tool to identify individuals at highest risk of life-threatening COVID-19.{*} Common genetic variants identify therapeutic targets for COVID-19 and individuals at high risk of severe disease.{*}
Table. 2.4.4. The HR, RR and/or OR of the of the death and preexisting conditions and comorbidities of the selected articles
Click on the picture to enlarge
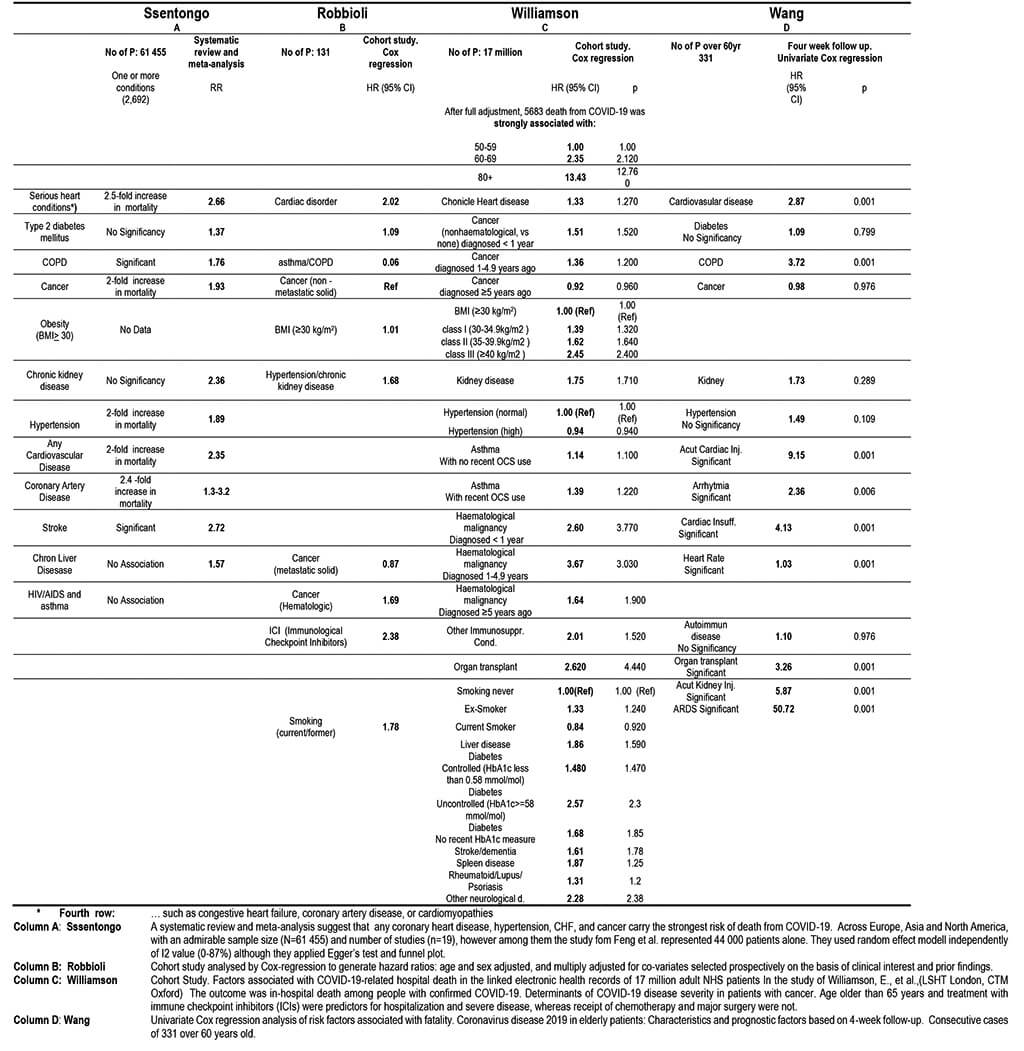


Fig. 2.4.4. Adjusted hazard ratio (95% CI) of death from covid-19 in men in derivation cohort, adjusted for variables shown, deprivation, and fractional polynomial terms for body mass index (BMI) and age. Model includes fractional polynomial terms for age (1 3) and BMI (−0.5 −0.5 ln (age)) and interaction terms between age terms and type 2 diabetes. Hazard ratio for type 2 diabetes reported at mean age. (QResearch database version 44; study period 24 January 2020 to 30 April 2020). Taken from ref. {*}
It has been well accepted that some comorbidities frequently coexist. For instance, diabetes{*} and COPD{*} frequently coexist with hypertension or coronary heart diseases.
Guan W.J., et al have verified the significantly escalated risk of poor prognosis in patients with two or more comorbidities compared with those who had no or only a single comorbidity. The hazard ratio (95% CI) was 1.79 (1.16–2.77) among patients with at least one comorbidity and 2.59 (1.61–4.17) among patients with two or more comorbidities. (p<0.05) Their findings implied that both the category and number of comorbidities should be taken into account when predicting the prognosis in patients with COVID-19. A thorough assessment of the coexisting comorbidities help to establish risk stratification of patients who more likely have poorer baseline well-being.
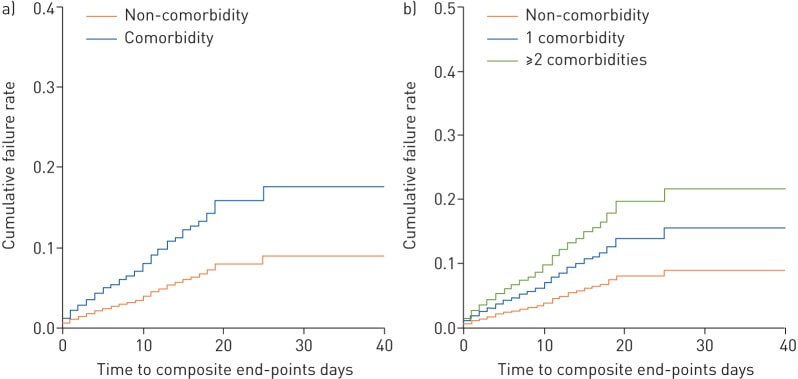
Fig. 2.4.5. a.) The time-dependent risk of reaching the composite endpoints between patients with or without any comorbidity. b) The time-dependent risk of reaching the composite endpoints (admission to intensive care unit, invasive ventilation or death) between patients without any comorbidity, patients with a single comorbidity and patients with two or more comorbidities. Taken from ref. {*}
The suggestion of this ELSE study for the determination of the selection criteria for the Vulnerable Population were screened and concluded through a critical and carefully selected system and multiply controlled workflow from the informations of the previous sections. (2.4.)
This ELSE suggestion should be
- carefully examined and verified concerning its validity
- confirmed its authenticity with even more up-to-date information
- improved, matured and professionally finalized
by a professional committee of cardiologists, diabetologists, oncologists and pulmonologists etc. of the WHO, CDC, Tessy and national health authorities, on the fall risk index based on age, comorbidities and other heath state parameters in order to determine the selection criteria for the VP.
The selection criteria would be highly modified according to the morbidity and mortality of the region, state, where it would be implemented. Similarly, important, the actual health care capacity in general and specific (ICU, ECMO, ventilators) capability of the given health care. Of course, from amoung the young population and the immunologically weakened population (immunosuppression, recently completed chemotherapy, etc.) should be included in the program, regardless of age.
The GPs should be involved from the very beginning of the process. As it was aforementioned previously, they should gain enough in-depth knowledge of the COVID-19 pathomechanism through further quick training. They have a particularly important role because they are personally familiar with patients therefore, they entitled in the final scoring in a range 0-5. The Table 2.5.1. below containes the the suggested final selection criteria scores based on the analysis of the previous sections.
Members of the VP would be further identified on the base of this predefined standard criteria, scheme, and index by GPs, who are personally familiar with them, resulting a surgically precision selection. Their work would be endorsmented with a number of supporting materials. In addition to the pre-developed scheme and index index, further professional team of the region would support the work of GPs with a number of associated materials. Thus, for example, based on pharmacy reception habits, an analysis broken down by settlements and frequency, and by disease, can be deduced from the professional composition of medicines. In addition, statistics from the multidirectional (demographics, settlement structure, special medical supervision of districts, logistics of sampling, etc.) can be used for fine-tuning.
Table 2.5.1.The suggested score system of ELSE by age and different preexisting conditions and comorbidities according to the potential contribution to ICU admission and/or death.
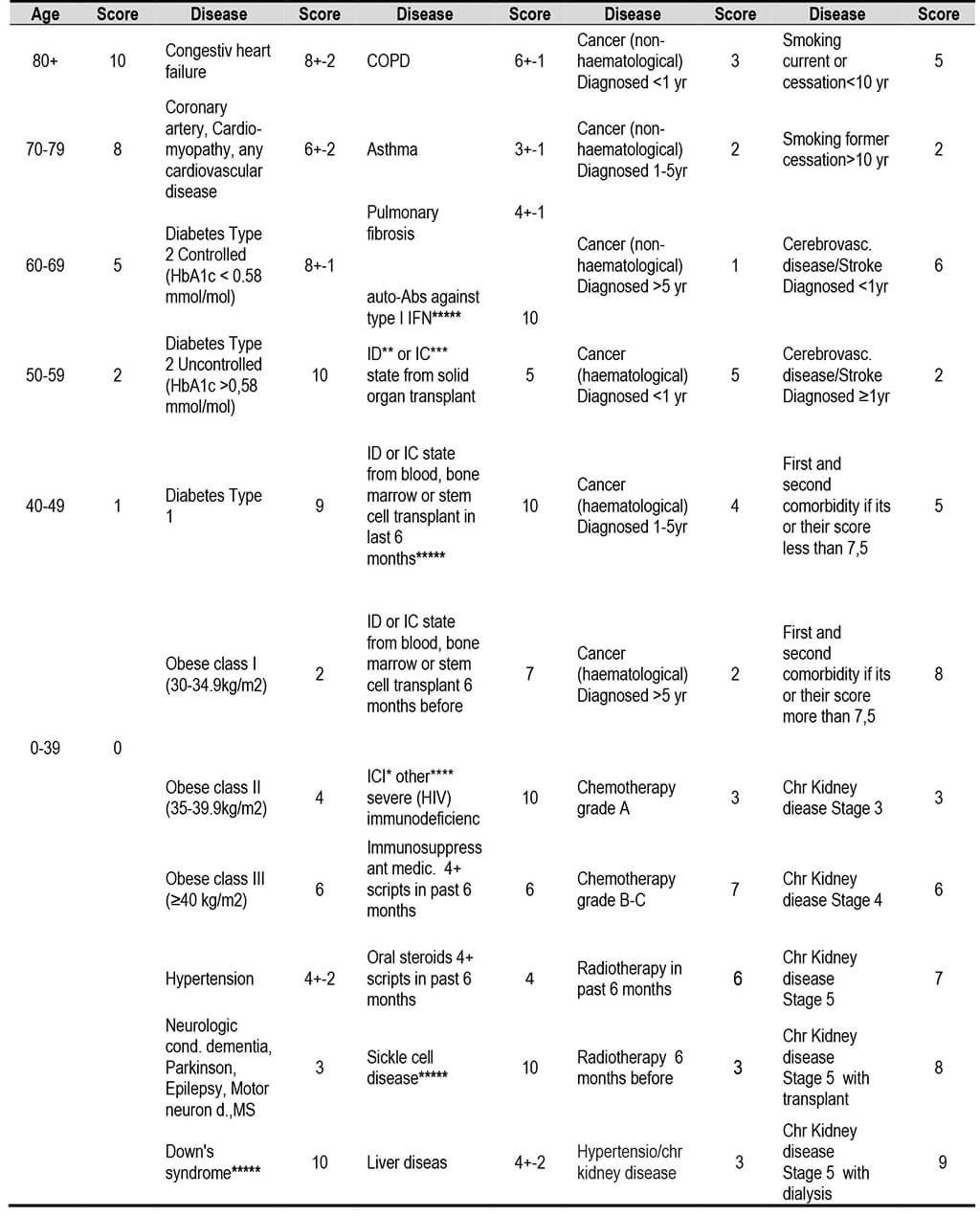
*ICI: Immun Checkpoint Inhibitor;{*} **ID: Immundeficiency; ***IC: Immuncompromised state; ****Other use of corticosteroid or other immun weakening medicines. *****INDEPENDENTLY of the SCORE ELIGIBLE in the FIRST LINE AMONG VP /auto-Abs against type I IFN: screening test for neutralizing immunoglobulin G (IgG) autoantibodies (auto-Abs) against type I interferon IFN (IFN-α and/or IFN-ω)/ {*} ID or IC state from blood, bone marrowe or stem cells transplant 6 mo before; Sickle cell disease; Down’s Syndrome;
The selection criteria would be highly modified according to the morbidity and mortality of the region, state, where it would be implemented. Similarly, important, the actual health care capacity in general and specific (ICU, ECMO, ventilators) capability of the given health care. Of course, from amoung the young population and the immunologically weakened population (immunosuppression, recently completed chemotherapy, etc.) should be included in the program, regardless of age.
The GPs should be involved from the very beginning of the process. As it was aforementioned previously, they should gain enough in-depth knowledge of the COVID-19 pathomechanism through further quick training. They have a particularly important role because they are personally familiar with patients therefore, they entitled in the final scoring in a range 0-5. The Table below containes the the suggested final selection criteria scores based on the analysis of this section.
Table 2.5.2. Five simulated examples of patients by the previous table. The simulated examples clearly demonstrate that VP can be personally delineated and identified using the ELSE method. This is not a superficial, rough, but a thoughtful, precise and purposeful approach. Sophisticated challenge recquires sophisticated solution. Note that “XT” with 85 yr (and diabetes, COPD, Hypertension) has less score, than “XY” with 68 yr; “XV” with 48 yr; and “XZ” with 38 yr.

Beyond health considerations, there may be other factors that need to be considered. For example, in the case of access to resorts and hotels, those living in densely populated multi-storey blocks should have an advantage over those living in a garden house, as transporting to the district, or even walking around the house in VPHQSB may pose an increased risk of infection.
Some other considerations, given that the primary cause of ICU cases and death is the severe acute respiratory syndrome:
- If Chronic respiratory disease is also present, this is the first comorbidity (Severe Acut Respiratory Syndrom precondition).
- If there is no Chronic respiratory disease but the Cardiovascular disease is present, then it is recommended to classify it as first comorbidity.
- Of course, the condition caused by a given comorbidity will override this classification offer, as if someone’s stage of cancer determines their prospects, they will receive the first comorbidity position.
- Among other things, this values the role of GPs, (eligible for 0-5 scores) since, they obviously know the patients personally, furthermore they are constantly treating and monitoring them.
- Importantly, GPs, professional staff and every other participant should be exempted from the possibility of a subsequent malpractice court case by appropriate legal provisions or takeover the responsibility.
Alternatively, prevent such incidents from occurring with statements made in advance by decent lawyers.
This section is essential in the ligth of the parametrization of the epidemic model. We should estimate the number of people, who requires intensive care
The section demonstrates also that regardless of the large number of elderly chronic conditions, a rational complex systematic approach allows the identification of COVID-19 related VPs.
This effective method applies multiple buffers, which also contribute to the development for the selection methods of the patients through ELSEs with their findings, ideas, and suggestions. Furthermore, this section of the article contributes to the most effective selection method of the vulnerable patients (VP) for authorities and countries, by unique insights, ideas, and proposals, who intend to apply the ELSE, anything before else.
Adapted from the chronic conditions among the US adults surveyed in 2012-2016 {*} Table 2.6.1.1.
The fatality rate in different age group showed a significant correlation with the number and types of existing chronic conditions. Some comorbidity has no relevant or identified impact on the fatality of COVID19 (such as hypertension and lipid disorders), while other, respiratory related diseases can risk the recovery significantly. An earlier published cross-sectional analysis surveyed the number of chronic conditions in the US population in different age groups According to this study in 2016, among the US adults, approximately half (49.8%, 117 million) had no chronic conditions. 24.3% had one out of ten selected chronic condition, 13.8% had two conditions, while 11.7% had three or more conditions in Table 2.6.1.1. upper third.
As was mentioned earlier, not all the chronic conditions have impact on the COVID, only asthma, diabetes, hypertonia, upper respiratory disease. In contrast to that mood disorders, arthritises, inflammatory joint disease does not add risk for the calculation of fatality. According to the study of, the most relevant disease, which have serious impact on the COVID-19 infection is the heart disease, asthma, diabetes, hypertonia and cholesterol related symptoms, and mood disorders arthritis can be exclude. Fig. 2.6.1.1.
This led us to decrease by 50% the vulnerable population (50% reduction). (Table 2.6.1.1. middle third)
Other studies reported less risk for lipid or cholesterol metabolic disorders, which lowers more the effect of comorbidities down to 20% (80% reduction). (Table 2.6.1.1. lower third). Consequently, in our study, the effect of COVID-19 related commodities was counted in the pandemic, so two scenarios were taken into account by the reduction of the number of exposed people by 50% and 80%, depending on the commordities considered. In the cases of 80% reduction, only the 20% of the 10 most important of commodities are calculated, and the lipid and cholesterol disorders were also excluded from the study. The effect of these comorbidities was questioned in several studies.
The probability of having multiple types of chronic conditions increased with age. On average, study participants had 2.34 types of chronic conditions, increasing by age from 1.88 types of chronic conditions per beneficiary aged 65 to 69 years to 2.71 types of chronic conditions among individuals aged 85 years and older.{*}
The estimation of the ICU/10k is based in the Table 2.6.1.1., which collected the estimated percentage and the number of US Adults with Chronic Conditions between the age of 18-100. The survey was done by National Health Interview in 2012. Considering the impacts of the various chronic conditions to the fatality rate of the COVID-19, we made two alternative calculations, where the numbers given were reduced by 50% and 80%, respectively to the collection of chronic condition. When only asthma, coronary and heart disease as well as diabetes mellitus were considered, we reducuced the number of vulnerable population by 80%. Including more chronic conditions, such as lipid disorders and the hypetension, we can reduce the original values by 50%.
Table 2.6.1.1. Estimated Percentage and Number of US Adults Aged ≥18 Years with Chronic Conditions by Select Characteristics, by National Health Interview Survey, 2012. Population in 1,000 (ppl k). Total 2012 US adult population: 234 million persons. (Ward.B.V. et al.).
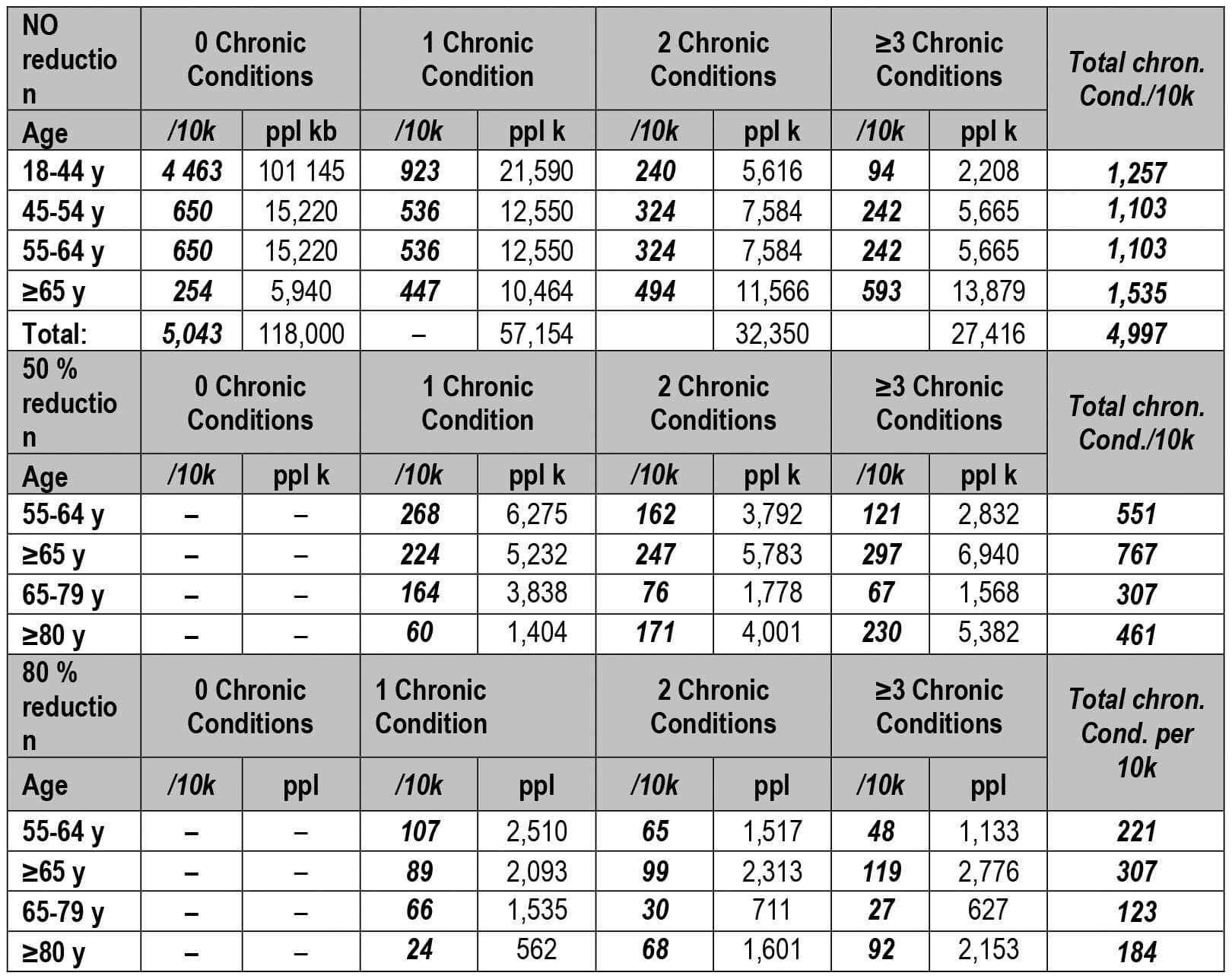
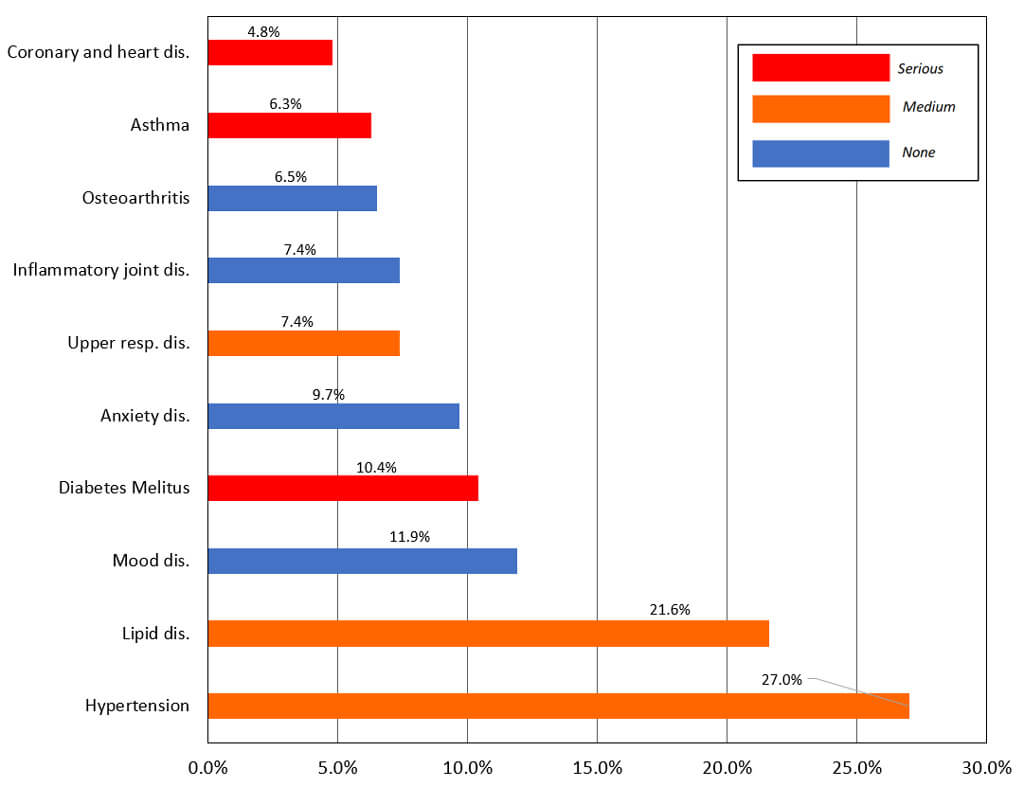
Figure 2.6.1.1. Prevalence of top chronic conditions among the US adults (in %), surveyed in 2014, adapted from Robert Wood Johnson Foundation and Johns Hopkins University. Taken from ref. {*}
Adapted from the chronic condition and defining the VP of the population at increased risk of severe COVID-19 due to underlying health conditions in global, regional, and national level in 2020.{*}
The aim of this study from excellent centers is to provide global, regional, and national estimates of the number of individuals at increased risk of severe COVID-19 as a result of their underlying medical conditions during 2020. The study estimated that 1·7 billion individuals, comprising 22% (15–28) of the global population, have at least one underlying condition that could increase their risk of severe COVID-19. This value does not include older individuals without underlying conditions. The prevalence of one or more conditions was approximately 10% by age 25 years, 33% by 50 years, and 66% by 70 years, and similar for males and females. The most prevalent conditions in those aged 50 years or older were chronic kidney disease, cardiovascular disease, chronic respiratory disease, and diabetes. They mapped the conditions listed in the Global Burden of Diseases, Risk Factors, and Injuries Study (GBD){*}
To lists of conditions associated with increased risk of severe COVID-19 from guidelines published by WHO and agencies in the UK and USA. The mapping was completed by a clinical epidemiologist (CW-G). Prevalence estimates were extracted by age, sex, and country and grouped into the following 11 categories: (1) cardiovascular disease, including cardiovascular disease caused by hypertension; (2) chronic kidney disease, including chronic kidney disease caused by hypertension; (3) chronic respiratory disease; (4) chronic liver disease; (5) diabetes; (6) cancers with direct immunosuppression; (7) cancers without direct immunosuppression, but with possible immunosuppression caused by treatment; (8) HIV/AIDS; (9) tuberculosis (excluding latent infections); (10) chronic neurological disorders; and (11) sickle cell disorders.
For multimorbidity adjustment the COVID-19-relevant categories were defined. This included cardiovascular disease (defined as the presence of one or more of coronary heart disease, hypertension, cerebrovascular disease, peripheral arterial disease, heart failure, or atrial fibrillation), chronic neurological disorders (defined as one or more of dementia, multiple sclerosis, and Parkinson's disease), and chronic respiratory disease (defined as one or both of chronic obstructive pulmonary disease and bronchiectasis). The remaining COVID-19-related conditions listed previously were counted separately. GBD provides separate estimates for hypertensive heart disease and chronic kidney disease due to hypertension, but it was not possible to make this distinction in the multimorbidity datasets, so all hypertension was included in the cardiovascular disease category.
However, trying to shield an excessive proportion of a population can strain country resources and reduce the overall effectiveness of shielding. A detailed assessment of the number of at-risk individuals can inform possible shielding strategies. Therefore, the study estimated the number of individuals at high risk, defined as those that would require hospital admission if infected, 4% (coresponding with the findings in the next 2.6.2. section) calculated using previously estimated age-specific infection–hospitalisation ratios for COVID-19. (Fig. 2.6.1.2 and Fig. 2.6.1.3.)
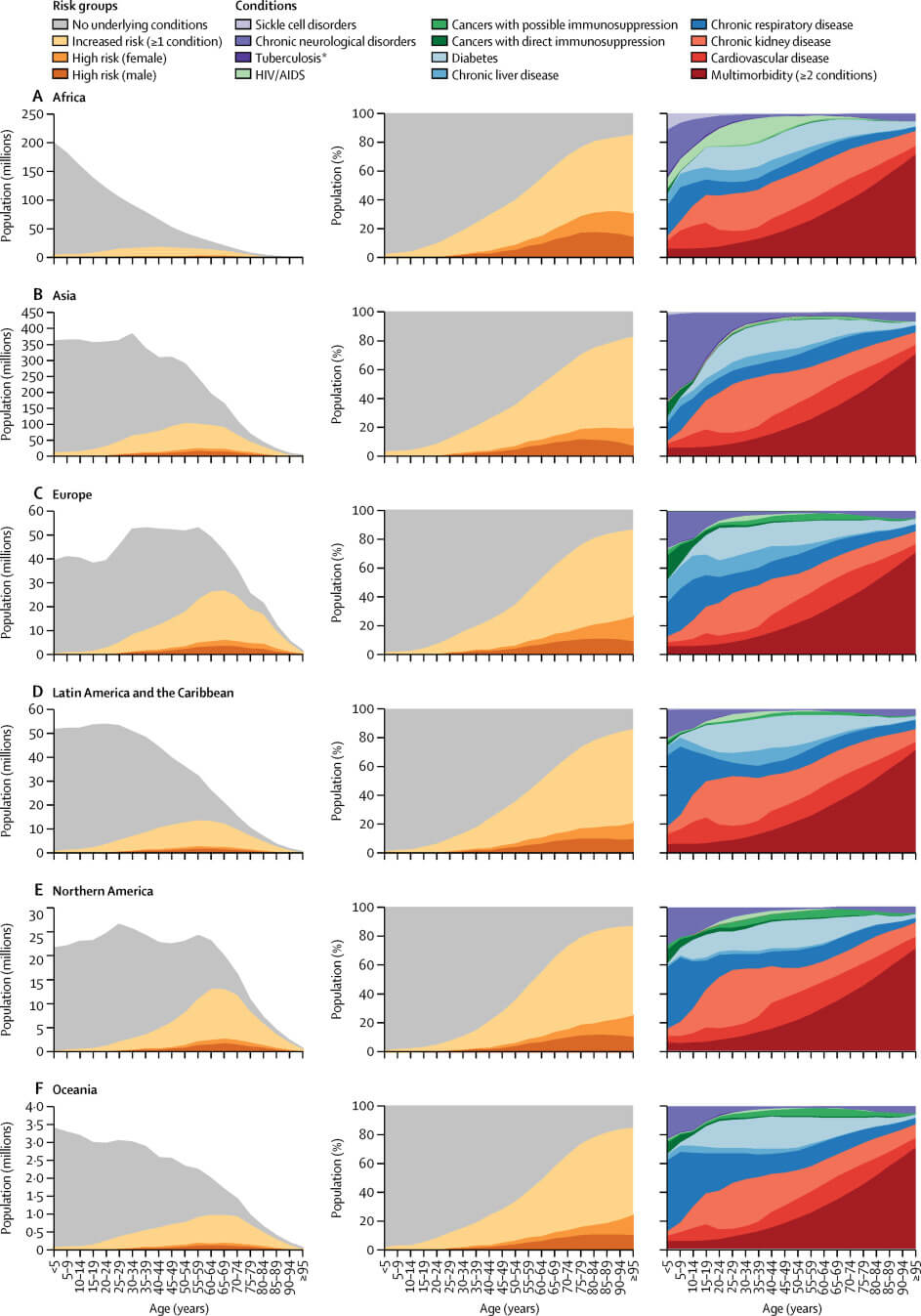
Figure 2.6.1.2. Proportion of risk groups and conditions of severe COVID-19. (Clark.A. et al.)
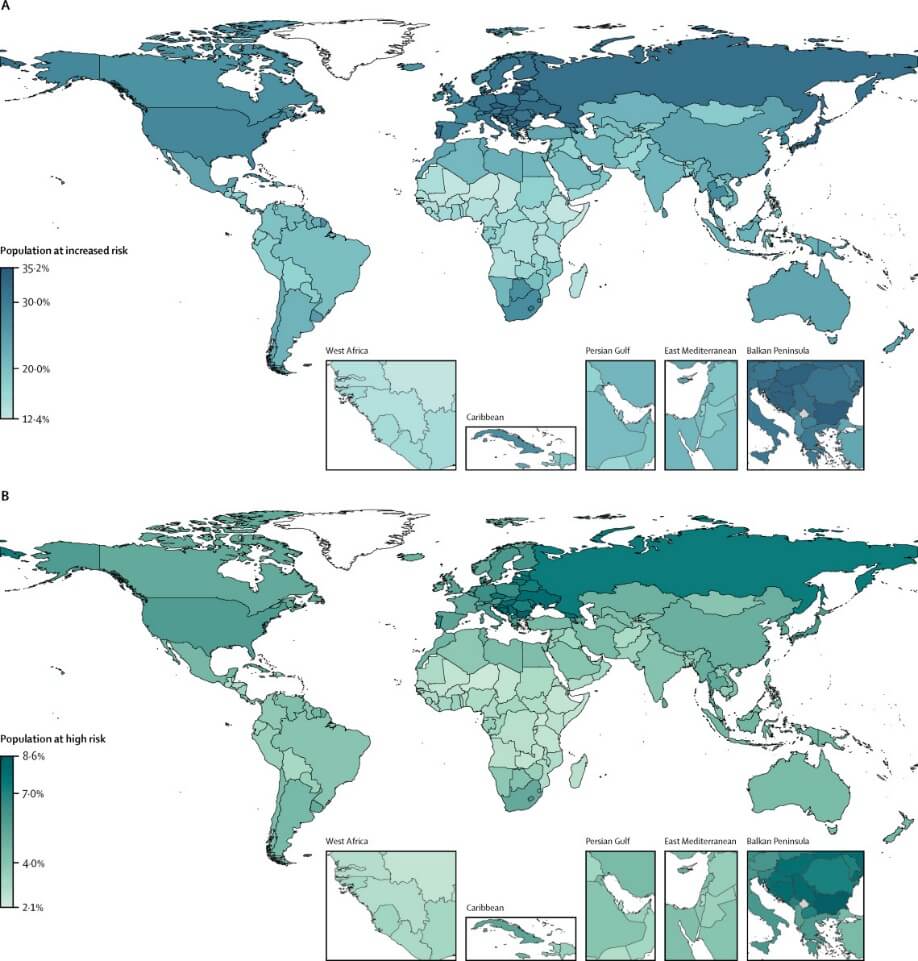
Figure 2.6.1.3. Proportion of population at increased risk and high risk of severe COVID-19 by country Clark.A. et al.
We estimated that 349 million (186–787) people, - 4% (3–9) of the global population — are at high risk of severe COVID-19 who would require hospital admission if infected.
For easier comparabibility of this article results and conclusions the presents study is based on all the data and parameters published by the Imperial College COVID-19 Response Team (Report 9) as default values. According to this the estimated R0 of 2.4, 81% of the ten million population would be infected. From the moderate, mild, or asymptomatic infections (95.6% of infections), 4.4% infections (350 000 patients) that lead to hospitalization but not critical care (3.08%), and infections that require critical care (1.32%)
Table 2.6.2.1. Current estimates of the severity of cases. The IFR estimates from Verity{*} et al. have been adjusted to account for a non-uniform attack rate giving an overall IFR of 0.9% (95% credible interval 0.4%-1.4%). Hospitalisation estimates were also adjusted in this way and scaled to match expected rates in the oldest age-group (80+ years) in a GB/US context. These estimates will be updated as more data accrue. Age-group (years) % symptomatic cases requiring hospitalisation % hospitalised cases requiring critical care Infection Fatality Ratio to account for a 75-80 % non-uniform attack rate giving an overall IFR of 0.9% (95% credible interval 0.4%-1.4%).

Table 2.6.2.2. Adapted from the Table 2.6.2.1. where the real number of the population projected to the Hungarian demographic data. (10M) ( 81% of the populations predicted to be infected over the course of the epidemic. 4.4% of infections that lead to hospitalization but not critical care (3.08%), and infections that require critical care (1.32%) R0 of 2.4, according to Imperial College Report-9). Summarize the number of Vulnerable Population (VP) and the predicted number of deaths in the different age groups are indicated by those cases requiring critical care (ICU). Age-group, requiring critical care Infection Fatality Ratio (IFR) to account for a 75-80 % non-uniform attack rate giving an overall IFR of 0.9% (95% credible interval 0.4%-1.4%) adjusted in this way and scaled to match expected rates in the oldest age-group (80+ years) in a GB/US context. The Table 2.6.2.1.also shows the number of VPs within each age group. The exact number needs to be clarified in each region on the basis of these guideline numbers. It is very important to understand that the scores of VP-selected patients can only be compared within each age group. Therefore, for example, for the 85+ age group, 78 / 10k is the number of comparable patients. The number and severity of VP patients aged 70-79 is 42/10k and the selection criterion can also be used only within this age group 70-79. The number of patients to be selected in a region (80+: 78 /10k, 70-79: 42/10k, 60-69: 18/10k, 50-59: 5/10k, 0-49: 2/10k) = 146/10k. (See chapter 3.4).

Table 2.6.2.2. cont.
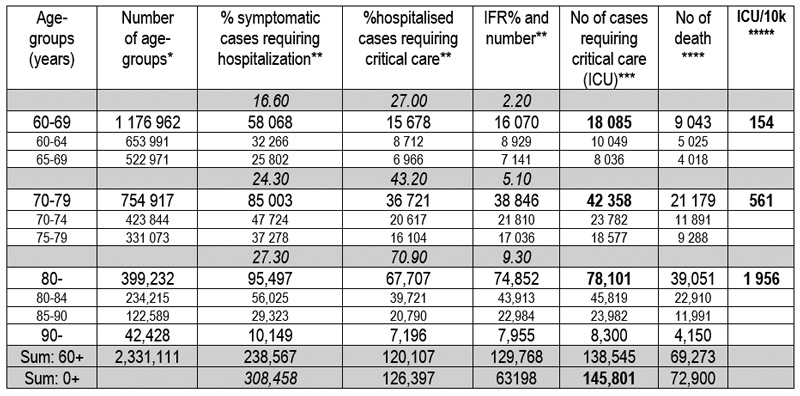
* Hungarian demographic data;
** No of cases derivatived from the Table 2.6.2.1. The gray line are data exactly
of the Table 2.6.2.1. in %;
***Number of Vulnerable Population (VP;
***Half of the Number of ICU cases;
*****The ICU/10k calculated from the previous data.
The primary reason for the next elaboration of this unexpected depth, going into even the smallest details, is that the article tries to prove undoubtedly to all skeptics that the infection-free, safe isolation of VP is feasible. It should also be emphasized that professional military logistics experts should execute the isolation.
Vulnerable Population can be isolated:
- separated from their home, in Cruise, Resort, Hotels (VPCRH)
- not separated from their home
- In Districts (VPD)
- In their own home (VPHQ and VPHQSB)
The isolation of VP – apart from metropolises and cities - also affects the following residential places, where special attention is needed: Although, as it is clearly proven in the next Chapter (Result 3), the VPCRH could be absolutely the only solution for managing this situation, like the dense areas of metrololities and cities.
- Villages
- Multigeneration areas
- Hospitals
- LTHF (Long Term Home Facilities including Nursing Homes)
If the opportunity starts on a voluntary basis, we can be sure that a significant number of volunteers will apply from the beginning.
The justification of VPCRH for the most suitable place to isolate VP.
Cruisers, Resorts and Hotels that are located in an isolated outdoor environment the most effective location for the VP.
A well-trained already inoculated i.e. protected staff candidates required, for - according the importance of the task – an adequate high salary.
The bottleneck is the start-up. That includes the transport, the initial operation and the associated isolation of VPs in terms of infection prevention. A military commander is the sole person responsible for such achievement. This is in accordance with the military legislation related to liability of the area designated to him or her. The commander executes a military order. Qualified, trained, committed, protected military members must perform the special initiate steps and the supervision of the VPCRH places in general as well as hygienic surveillance. They should be protected by vaccination. During the transport they should ensure the protection against infection and in the new places adapt the guideline logistical of the physical movement, professionally put the operation in place and at the same time train the new protected groups of staff and leave the maintenance task for them.
The VPCRH can use for all of the VP candidates to quarantine, especially from the densely populated, inner areas of large cities, nursing homes, villages as well as the multi-generated areas to solve the isolation. In fact, if the VP stays in VPCRH until the critical months, even a year along with the use of the correct level of services, which satisfied them, the willingness of potential participants will increase. Thus, the VPCRH maybe solve the overwhelming majority, most probable the total of the expected needs. The capacity of these places abundant with the suggested 600/10k or even 1 000/10k excess number of candidates.
Cruisers: The Noah’s Ark cruisers seem to be the best choice for immediate deployment. From the outset, Cruisers are designed for rare contact with the outside world, such as the occasional port material intake (municipality). Before boarding cruisers, it is advisable to collect them in hotels in advance and test them continuously. Or if they are boarded directly it is advisable for the Cruiser to stay in the homeport for at least 2-3 weeks prior to departure to be sure of virus free environment of the ship. After that, there will open a larger opportunity in terms of both capacity and the variety and quality of the service. Professional military units train the protected staff for the hygienic rules, and protocols in case of infection and after that, the “steamers” can set off to the variety of locations. These purposefully prepared places (can be even Hawaii, Maldives, and Canaries etc) will receive them in the safe isolated environment. After that, the cruisers can return for transporting the next 5 000 VP group.
Resorts and Hotels: Those resorts and hotels that are located in a suitable environment where the isolation of them, (preferably in groups such as Coastal Peninsula Hotel Chains) are ideal. In-site logistics (patient movement, contact of non-protected staff with patients are detailed below. These require completely custom planning, logistics, and many other constrains.
The capacity of hotels in the US:
| From upper midscale to luxury: | 2,7 millions | = 5,2 million persons (two persons/room) | = 226/10k. |
| Total: | 5,4 millions | = 10,8 persons (two person/room) | = 470/10k |
Combining the options can even make isolation really enjoyable. Vulnerable Population of Cruisers and Resorts, for example, can rotate every two to three months. Even isolated islands (Maldives) – with protected staff - can be included in this cycle especiallyt if if it works in an internationally coordinated way.
Related financial principles:
- Assuming that a cruise/hotel / resort is, say, 70% profitable relative to the list price, let us take into account the fact that occupancy is currently 30% in this epidemic. Therefore, if the occupancy rate is 100%, then 50% of the list price should already be right for the operators. The more VP the state allows, the better the currently unused resorts and hotels will be utilized.
- VPs pay for example 5-10% self contribution, - or nothing - the rest is covered by the state up to the agreed 50%. The state pays a standard quota of about a margin between 10 (deductible) – or zero - and 50% of the average of the lower price resorts as a standard contribution.
- Nevertheless, for those, who are willing to pay deductible – or more deductible – for higher quality of VPCRH places, need to create an opportunity for them because this would allow to expand the capacity, In this way the more luxurian VPCRH places also will be rendered to isolate the VP. That can be very important, therefore, additional contribution recommended over the standard quota to fulfill the demands of enough VPCRH places. (See Table 2.1.7.1-4)
- The VPD, VPHQ and especially EMHQBS and over other NPI probable is the most affordable expense in low-income countries.
- To quantify the mean daily cost of intensive care, the results of a retrospective multicenter (253 geographically diverse U.S. hospitals) cohort analysis using data from NDCHealth's Hospital Patient Level Database, included 51,009 patients >/=18 yrs of age were as follows. Mean intensive care unit cost and length of stay were 31,574$ and 14.4 days (2,192$/day) for patients requiring mechanical ventilation and 12,931$ and 8.5 days (1,521$/day) for those not requiring mechanical ventilation.{*}
- According to the Fair Health Brief on the basis of IIR, the total average charge per COVID-19 patient requiring an inpatient stay is $73,300 and the total average estimated allowed amount per commercially insured patient is $38,221. On the basis of DRG, the per-patient average costs for hospitalized COVID-19 patients vary depending on severity. The total average charges per patient range from $74,310 for patients with major complication or comorbidity (indicated by DRG code 193), to $42,486 for patients with no complication or comorbidity (indicated by DRG code 195). The total average estimated allowed amounts per commercially insured patient range from $38,755 for DRG 193 to $21,936 for DRG 195.{*} Fig. 2.7.1.
- Hospital costs, such as facility fees, represent about 90% of the cost of inpatient admissions for large group enrollees treated for pneumonia or those in need of ventilation due to respiratory illness. For those requiring ventilation, the remaining physician fees average over $3,000 for an admission with less than 96 hours of ventilation and over $9,000 dollar when the patient requires more than 96 hours of ventilation. People with employer coverage who are admitted for COVID-19 treatment could face out-of-pocket costs exceeding $1,300 PLUS Potential surprise billing.
- There is also considerable variation in the cost of admissions for respiratory conditions. For patients who require ventilator support, the combination of longer stays and higher intensity treatments results in higher average spending. The median total cost of an admission for a respiratory condition requiring 96 hours or more of ventilation is $88,114 dollars, compared to $34,225 for an admission requiring less than 96 hours of ventilation. The VP certainly are in a respiratory condition.
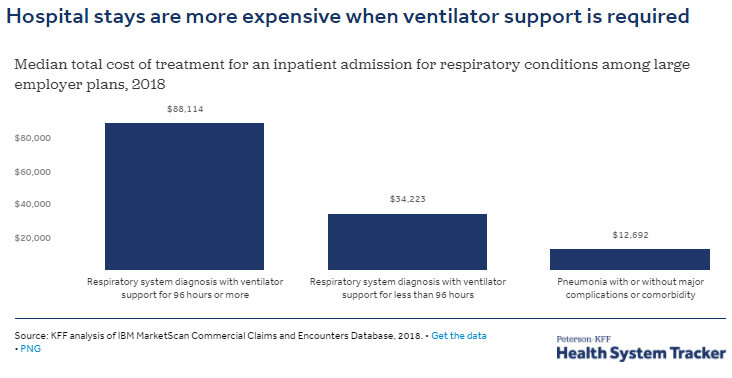
Fig. 2.7.1. Taken from ref {*}
- The COVID-19 related ICU stay range from 5-19 days (120-456 hours){*} A patient with ARDS caused by other illnesses might rely on ventillator for 7 to 10 days, but some coronavirus patients require more than 2 weeks.{*} For two cohorts, patients ventilated from the admission had an expected duration of ventilation (12.25*, 14.57** days), with a higher risk of death (54%* and 20%**).{*} Concluding from the data, VP’s health funding is not just $ 88,000, (requiring 96 hours – 4 days ) more likely 12-14 days to be $ 250,000 - $ 300,000.
The fee paid by the state for VPCRH’s accommodation and services will be reimbursed to the state on the order of magnitude, compared to the cost safe on the side of the health care system. Not only the higher cost of ICU, but saving lives and the inestimable significance of the socioeconomic restarting. Aggregate indicators can take into account. (employment, industry recovery, reduction in deaths in hot spots, and improvement in impressive indicators such as the recovery of society, the ray of hope for recovery from the hopeless situation, etc.) In any case, this type of “grant” costs significantly less than the ICU treatment of those VP, not to mentioned immeasurable current donation to the whole impaired socioeconomy.
We proved, that the ELSE-VP strategy, irrespectively of the fine details, is a very powerful procedure in the hand of any government to minimize the number of deaths and reasonable reducing the duration. However, beside the epidemic management, we cannot ignore the financial aspects for two reasons. At first, the government budget must be controlled, strictly against the overspending, even under normal condition. Secondly, the current pandemic caused a significant (ca. 10-20%) drop in the governmental income of most of the country, due to the depletion of the economy.
According to a widespread cost estimation, the cost of the critical care, including the maintenance of the ventilation/respiratory capacity, is very high in the governmental budget. It was estimated that the total cost can be as high as 80 thousand of USD for one patient, irrespectively that he or she survive or not. An ordinary intensive care unit without ventilation is costing around 30 thousand USD. Using the original population distribution between the four age groups (AG1–4, see Table 2.7.1.1. 2nd, 3th columns), we can estimate the VP population (Table 2.7.1.1 4th and 6th column) according to age groups by predefined ICU/10k. This is resulting the predicted cost of the direct Natural Outbreak (No of death: 72/10k Icu burden: 144/10k) without preventive measures where the total cost is exceeding the 10 billion USD. (In Table 1 the 2nd row with 130/10k is already exceed the 10 billion $ number)
Table 2.7.1.1. The estimated financial burden of the medical treatment for VP in AG1–AG4, presenting in 8 sequences.
| The first row illustrate | the No of VP/10k | who need ICU (death rate is 50%) in | AG1-AG2-AG3. |
| The second row is | the No of VP/10k | who still require intensive care without death in | AG1-AG2-AG3. |
| The third row is | the No of VP/10k | who need ICU (death rate is 50%) in | AG4. |
| The fourth row is | the No of VP/10k | who still require intensive care without death in | AG4 |
| The fifth rows is | the No of VP/10k | who probable need intensive care in | AG1-AG2-AG3 |
| The 6.-7. rows are | the No of VP/10k | who may need intensive care at a lower cost in | AG1-AG2-AG3 |
| The eighth rows is | the No of VP/10k | who probable need intensive care in | AG4 |

athe cost of ventilation 80 kUSD per person;
bthe cost of intensive care 30 kUSD per person;
c If we calculate the more realistic 250 000- 300 000$/person (page 54 ref: 39-40)
the cumulative cost for the 559 VP/ 10k would be around 150 000 000$ (row 8/b)
instead of 38 220 000$ (row 8);
d AG1-3 = VP(0-79) and AG4 = VP80+
As it was demonstrated in a previous section, the most effective isolation of the VP can be carried out at existing cruiser ships, resorts, and hotels, which are almost empty during the epidemic. A very convenient calculation, including a low-price accommodation (100 USD/person), presented in Table 2.7.1.2. can lead to the conclusion, that the overall price of the isolation of one person is as cheap as 10 000 $ for 100 days and 36 500 $ for one year. In this case, of low-price, the government should cover all the expenses, however, because this cost includes only basic service, it is hoped that the population at large will accept this.
For the VP and excess buffer, I-II, who can afford a more exclusive (high-price) category can be also introduced, where the government covers the basic service, and the half of the additional cost must be covered by their own (resulting an overall 25% self- and 75% governmental contribution).
In order to reach the sufficient excess number of people and saturate the accommodations, this isolation can be offered for not only the strictly VP people, but those who are in the 6th or 7th row of the excess III-IV. (Table 1/B/1). For them, a very convenient, conservative price calculation is suggested, for example for the low-priced bed it demands only 15% self-contribution and 85% government support. The same is true for the high-priced category, but there the self-contribution is already 50%. A one-year calculation is also presented in Table 2.7.1.2.
Table 2.7.1.2.. Cost distribution of the low and high price accommodation.
Self-contribution and governmental support.

This cost calculation undoubtedly proves that the isolation of the VP, even with excess, means significantly lower overall cost (ca. 50% 20 billions vs 38 billions USD/pers), than the estimated cost of the health care, if we do not isolate the VP during the pandemic. In the case of high accommodational price, the cost of the health care and the cost of accommodation are close to each other. In the mirror of the more realistic 150 billions, the comparison is more evident. Not mentioning the relieving effect to the whole economy. In addition, we should highlight that in the frame of VP protocol, we save a significant number of lives for their family, which is uncountable from any point of view.
Table 2.7.1.3. The estimated financial cost of the isolation of VP and the suggested saturation of VP capacity

It is possible for cruisers, resorts and hotels to be organized privately with public support, in addition to the above, for individuals who want to spend this transition period at ease due to their sense of security and / or fear. The transport of VPs would be provided by the state (military serice). From now on, protected staff and continuous isolation would be provided by the reception place. Operations would take place under appropriate contractual and insurance conditions based on official health guides. Obviously, since people work until the age of 60, little occupation is expected in the 40-59 age group. This of course would proceed by governmental support. Table 2.7.1.4.
Table 2.7.1.4. Suggestion for governmental support by age stratification:
| AGE | Gov. contribution High Price | Gov. contribution Low Price |
| 80+ | 50% | 65% |
| 70-79 | 40% | 55% |
| 60-69 | 30% | 45% |
| 50-59 | 20% | 35% |
| 40-49 | 10% | 25% |
VPCRH, VPDistrict, VPHQ (2.9.2.) should also be provided for those who strictly not belong to a VP since this possibility cannot be denied ethically from them, for the reason that it is not possible to predict when a safe vaccine will be developed which will prevent death. Until their lives are in danger, which could raises serious ethical question. This is possible by the excess buffer capacity from 72/10k up to 600/10k.
- If the opportunity to be isolated in the resorts starts on a voluntary basis, it is certain that a significant number of volunteers will apply from the beginning and will then become increasingly popular, especially as it with the appearance of the vaccine, the death rate will be higher, than before.
- Due to the proliferation of resorts and districts, a mutually reinforcing circulus viciosus vica versa feed-back mechanism can be expected to:
- First, then it turns out that there are no deaths due to the military discipline in the resorts.
- In this way, the young working generation will exert pressure on the elderly to make use of to take advantage of it.
- Decision makers decide to lift up the restrictive measures, considering the majority public pressure and provide more and more the opportunity for VPs.
- Since the growing Re value, for potential VP, the out-of-home environment becomes a progressively increasingly dangerous target shooting range, forcing them to choose to the safest and most comfortable resorts those will be increasingly saturated.
- Later if the VPCRH capacity overloaded, only the less comfort districts VPD and VPHQ may remain for them.
Recommendations to be considered to minimize the potential infection in the VPCRH protocol. (see 6.1. Appendix 1)
If for any reason the VPCRH are saturated or can not be a choice the VPD are the next option. The isolation of VP will last during a couple of months until the appropriate level of protection HI is developed. This period cannot be tolerated between indoors. Therefore, sufficient number of open districts would be set up countrywide, which allows to isolate not only the directly affected 0,7 % but up to 6 % of the population, rendering a safe buffer for the potential fatal cases and defending of the feeling of exclusion and fear of death of other elderlies. Important, that the strictly organized and isolated milieu should create in every season a more comfortable and enjoyable atmosphere and a more pleasant lifestyle, even as it was before.
The designation of possible districts obviously depends on local characteristics. This is a function of the geographical, labyrinthine logistics, and physical capacity of the patient population for the functional radius of a given area. Municipality and local police can help in the designation.
Table A.2.1. and Table. A.2.2. in Appendix 2. (6.2.) indicate the possible number of patients in the districts, demonstrating the accomodation of 250-350-500 VP persons/ district.
It should be taken account that not only the active but the dismantled soldiers, even who are now in pension volunteers can also be rendered for the task. Their number depends on the number of districts, the number of VP/district and their further tasks related the VPCRH, LTFC, MMI (military mobile units) and so an.
The required soldiers is calculated in the Table A.3. in Appendix 3. (6.3)
As over and over again in this chapter the author likewise desires to prove the Armed Forces will protect the country from any attack. This is their job at present. The current enemy is now uniformed, little creatures who are attacking our country in an unorthodox way. The US president also compared the attack on viruses as a war.{*}
The main transporters are, of course, directional buses. Anyone who cannot move on foot or is too far away will be transported by military passenger carriers. Between panel houses, military jeeps or minibuses may be more efficient. Routes to outdoor locations should be designated. Positions where the movement of the Vulnerable population can be controlled should be identified (e.g. check for unavoidable intersections where the risk of contact with the outside world is increased, paying more attention).
- Appendix 4. The detailed instruction of transport of the VPD
- Appendix 5. Table A.5. shows the average number of seats
- Appendix 6. Table A.6. shows the optimal use of buses
Protocol in case of infection
- All the VPs are strictly locked up in their residence for 14 days, contact is not allowed, food, etc. is provided for them. Outside walking is allowed with military personal attendance.
- Those who have symptoms be hospitalized.
- After 14 days and testing, after that those elderlies who have no symptoms will return to the district life.
Before any further analysis would continue, let make it clear, the obvious solution is the isolation of the VP (VPCRH) from the nursing homes. They are much more identificable and their percentage significantly higher than in the average population.
As over and over again in this chapter the author likewise desires to urges everyone that over the scientific part of this article, do not to express an opinion on the feasibility of the isolation. Only high ranked logistical military experts are entitled to do so. This is a technical part that cannot be swept off the table by a simple superficial opinion.
As it is detailed in 2.6.1. the recovered therefore protected number of the population should exceed the 1/3 of the total population (WHO {*} and CDC {*} that offers and extraordinary abundant well-trained staff candidates, for an adequate high salaries.
In 15 600 nursing home 1,3 million residents, 0,5% of America’s population lives in long-term care facilities,{*} but as of August 27, 2020, this tiny fraction of the country accounts for 43% of US COVID-19 deaths.{*} The situation is similar in Sweden, although the managing of every day operation is out of control of the authorities. In case of infection the problem is difficult in Germany and Hungary, too.
The policies implemented in nine long-term care facilities in King County, is a proof that the invading of COVID-19 can be stopped. With the active surveillance for potentially infected staff, patients, visitors and with the appropriate employing proactive steps of control measures{*} the one third of death in the US{*} could have been prevented. The nursing home can only be considered as a natural shelter that are not treated properly. The soldiers and the corresponding protocol should manage it like a pre-existing VP distric. According to WHO – if not indicated to transfer to hospital - confirmed patients can be isolated and cared for at the LTCF.{*}
In Nursing homes as in dense inner-city environment, the VPCRH version of VP protocol should apply. If it is not mandatory and for the reason that of volunteering, many VP candidates maybe want to stay in the Nursing home residency. In this case the following options remain: The guidance for LTCF and chronic hospital departments (as it is introduced by the author in the Szent Donat hospital (Hungary) elderly/chron department including 300 patients. (https://www.raczt.hu/ (Appendix 7). Similarly, the regulations introduced in nursing homes in Japan are strict. Its effectiveness appears to be significant, as is the situation in the US and Sweden. Japan has the world’s oldest population. Yet it evaded a coronavirus crisis at elder-care facilities.{*}
As in Nursing homes or dense inner-city environment, the VPCRH version of VP protocol should apply. If it is not mandatory and for the reason that of volunteering, many VP candidates could stay in the Multigeneration environment. In this case, the VPHQBS of the VP Protocol could offer with low (70-75%) or probably less efficiency.
The household is a key context for COVID-19 transmission. The average size of households that have a resident over the age of 65 years is substantially higher in countries with lower income{*} compared with middle- and high-income countries, increasing the potential for spread generally but also specifically to this particularly vulnerable age-group. Contact patterns between age-groups also differ by country; in high-income settings contact patterns tend to decline steeply with age. This effect is more moderate in middle-income settings and disappears in low-income settings.{*} The 21% of older than 65 year live in a multigenerational household.{*} Among them the Vulnerable Population 65+ is 21/10k (0,21%/ppl) over 50+ is 26/10k.{*} The task is to isolate these 26 patients from ten thousand inhabitants. Here is why it will work to just isolate the elderly and vulnerable instead of not.{*} They just simply should isolate to the VPCRH version of the VP protocol.
As in Nursing homes, Multigeneration or dense inner-city environment the VPCRH version of VP protocol should apply. If it is not mandatory and for the reason that of volunteering or lack of VPCRH capacity, therefore many VP candidates could stay in the village, then analysing the circumstances, establishing districts in villages is not taken into account due to the following:
- Logistics is completely different.
- The concept of outdoor space in villages cannot be interpreted. There is no claustrophobia like feeling from the confined flat. No need to relieving.
- The number of military personnel would increase disproportionately.
- Settlements of a few hundred can be considered as a quarantine in themselves, especially if the rules are followed.
Villagers will have much more human logistics and health resources by reallocating resources to ensure surveillance of austerity measures in settlements larger than 10K by untying the measures. Such vigilance and readiness, based on advance preparedness comparable to an expected military-military action, the rapid, determined military implementation of action on the basis of strict protocol guidelines, can provide a similar level of protection for the elderly living there as members of the VP. If anyone is willing to move near a VP area or live within reach of the VP area, of course they can be a member of the VP. From an epidemiological point of view the village acts as a cluster, where, - after the isolating of the VP to the VPCRH – the contact tracers has a role in detecting SSE who can be “transferred” to another village to develop faster and evenly the HI, preventing the geographically white spots. (See “Strategy for the eradication of SARS-CoV in Introduction 1/A).
If an infection occurs, then
- The special mobile military unit is withdrawn, and the elderly are strictly locked up in their residence for 14 days, contact is not allowed, food, etc. is provided for them.
- After 14 days of testing, those VP who have no symptoms will join mandatory to VPCRH
- Those who have symptoms will stay at home or be hospitalized, depending on the seriousness of symptoms.
- The infected person - if he does not require hospital treatment and especially if he is young - stays in the village to further infect the no-risk population in order to make them to be protected.
- We allow the village to become further infected, we do not close school, and they even get in more intensive contact, in order to develop immunity in more and more recovered individuals.
This article clearly demonstrates, that the feasability of isolation and protection from infection of this vulnerable population can be safely achieved by describing the implementation in both depth and minor details. The primary reason for the following elaboration with such depth, which goes even into minor details, is that the author is trying to prove that the task is feasible!
The scenario describes a series of steps that are gradually structured and should base on an accepted social consensus. This means that following the decision the media experts need to plan how to build up the communication and should start as possible.
Accuracy associated with the protection of the VP is the first priority. It is equally important to preserve the long-term tolerance of the VP. This is linked to the long-term sustainability of the austerity. The social life subsequently would return in two months, but during that time the herd immunity formation and control of the processes would continue for several months, which may extend through severel months. Therefore, it is especially important to create a comfortable milieu and an enjoyable atmosphere, which offer a more pleasant lifestyle for them, even compared to as it was before. If the conditions is terminated, they should remember this period with longing nostalgia. In fact, this can be an origin a tradition for them in the future, without soldiers, regular good atmosphere, meetings with community events enriched with a variety of programs, by the organization of local governments. The scenario: the elements of this proposal can be implemented in a shorter period of time. As the individual divisions operate independently as well as the specific tasks of varying difficulty degrees of complexity are, the deadline is determined to be brisk work, but it must be performed precisely and all the elements of the secure start to be prepared properly. The detailed Scenario is in the Appendix 8.
This section can be found in Appendix 9.
The United States has about 3.6 ICU beds per 10,000 people aged 16 and older. Of course, the numbers vary differently by regions, (Fort Collins, Colo. 1/10k to Slidell, La., region 11/10k) the ICU occupancy rate is around 62%. This rate can push down to 45% or less with moving of the ICU’s mild cases to regular beds, resulting of a 2,0 ICU beds per 10,000 people. If the rate is pushed down to 30% or less with moving of the ICU’s mild cases to regular beds, resulting of a 2,5 ICU beds per 10,000 people.{*} So if 3.6 / 10k capacity means 2 000 excess beds for COVID-19, then where the real capacity is 1/10k, the excess beds would be only 555 and the contrary where the capacity is 5,4/10k, the excess beds would be 3 000.
In a study the estimated number of ventilators is fortunately even more, 4,2/10k being an important bottleneck of ICU performance. Another would be the ECMO, which aggregated physiological effect with the ventillators, related COVID-19 is unavaible. But we have good reason to estimates the overall effect of ICU beds, Ventilators and ECMO expressing in the model only as ICU beds the number of 2,5/10k than the 2,0/10k. So, we tend to investigate situation in either 1,5/10k, 2,0/10k and 2,5/10k, because the compensating and balancing effect of ventillators, ECMOs, the pushing of the occupancy rate (between 55-70%) and the inter county, inter state transport makes it possible.{*}
The map{*} of the ICU beds need based on the data of the Harvard Global Health Institute,{*} shows that the majority of states (especially from the 100th longitude to the east but the west coast is good enough) with below-average ICU beds are surrounded by states with above-average ICU beds, whereby the ambulance transport the balancing is largely solvable.
Since the first wave the increased preparation resulted similar ICU assets in Europe, too.
Imperial College COVID-19 Response Team in Report-9 measured the relative impact of five different non-pharmaceutical interventions (NPI). Among the mitigation strategy the Case Isolation (CI) in the home, Voluntary Home Quarantine (HQ) (for three-month, identification of a symptomatic case, all contacts in the community reduce by 75%. Assume 50% of household comply with the policy) and Social Distancing of those over 70 years of age (SDO) (for four months, reduce contacts by 50% in workplaces, reduce community contacts by 75% and 75% compliance) implemented in combination resulted 67%–81% reduction in peak ICU bed demand and 49–50% reduction of total death. (R0 = 2.4) {*} The other NPI’s reductions of total death are as follows: PC (school closer) 2%, HQ: 31%. The estimated overall impact based on Report 9 could be adapted to the actual epidemic environment.
Table 2.9.1. Traditional and ELSE NPI.
| NPI | NPI impact | Comments | Referents |
| PC (alone) | (2%) | Imp. Coll. | Imp. Coll.: Report-9 |
| Mask | 20-30% | IHME | IHME{*} Nature{*} |
| New bus (transport) and shopping system | 10-20% | ELSE* | |
| Home delivery by municipality | 10-20% | ELSE* | |
| SDO | 20% | Imp. Coll. | Imp. Coll.: Report-9 |
| Habitual behavior due to the measures | 10-40% | Imp. Coll. | Imp. Coll.: Report-26{*} |
| HQ | 31% | Imp. Coll. | Imp. Coll.: Report-9 |
| HQSD | 33-51% | Imp. Coll. | Imp. Coll.: Report-9 |
| HQSDO70+ | 67-81% | Imp. Coll. | Imp. Coll.: Report-9 |
| Swiss cheese pandemic model | 70% | Comb.of all NPI | Ian Mackay{*} |
| (EM)HQSB | 85% | ELSE** | |
| VPHQSB | 70-85% | ELSE** | |
| VPHQ | 90% | ELSE** | |
| VPHQ*** | 95% | ELSE** | |
| VPCRH/VPD | 95% | ELSE** | |
| VPCRH/VPD*** | 98% | ELSE** |
HQ =Home quarantine; PC =School Closure; SDO = Social Distance of Oldies; SB = dedicated Shop and Bus; *No military control; ** Military control; *** for doubled excess of VP;
In our ELSE model, we apply a special combination of NPIs. The HQSB+ employs NPIs, where the effectiveness of HQ is greatly enhanced for any age group supplemented by additional simple regulations. The regulations were adapted from the Report-9 and the identification of the certain age groups are the same. The letter “B” = Bus, which means one cannot use the public transport, which is the major motivation to leave home. The only expectation is the dedicated buses in predefined time-zone or nonstop toward and backward dedicated shops. The bus services include a regular disinfection and ventilation several times a day. The letter “S” = Shop means the restriction of the shopping expect in dedicated time zone or nonstop in dedicated shops. Shops and supermarkets have periodic daily – or much more effective nonstop i.e. 7-19 hr - opening and closing time intervals, and during closure, the interior is disinfected and ventilated.
Table 2.9.2. Several scenarios and the corresponding NPI values. The sum of the contributed values cannot exceed 100%
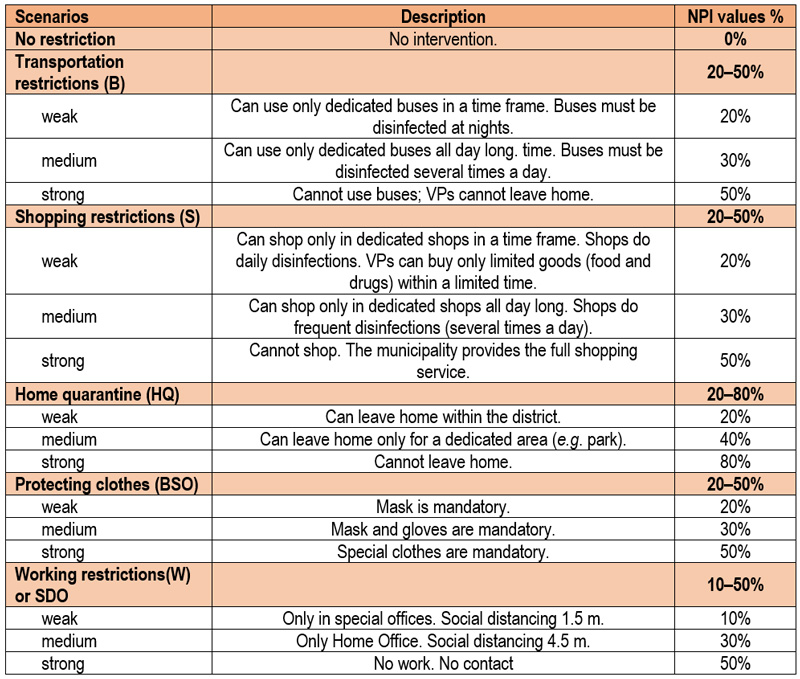
Example: HQSB (weak): 10%+10%+10%+10% = 40%
Regarding the use of the mask, the author recommends spraying the mask every few hours with silver colloid. He also introduced thismethod in his hospital (https://www.raczt.hu St. Donat Hospital). Although we were unable to perform a double-blind experiment, based on the common sense, the silver, which precipitates on the braids of a mask, through the well-known virucidal effect, should have only a beneficial effect. This may also have contributed to the fact that by January 2021 (the date of their vaccination), 60% of nurses close to the patient had become naturally infected, yet only 6 patients had developed COVID-19 since March 2020. They were treated according to the in-hospital quarantine protocol. This is a particularly low value for a 300-bed hospital.
According to the author, shopping malls should not narrow, but expand opening hours, e.g., from 5 to 24 hours. It is necessary to limit the number of people staying at the same time and to paint distance signs in front of the payment counters, etc. Similarly, working and school hours (e.g. 7-10 / 11-14 / 14-18 year old students separately) start and end to spread out so that the load on public transport should be even and crowding should be reduced.
In addition to the low number of deaths, this protocol promotes the development of adequate HI, which in itself can eradicate the virus but most effectively boosted by the proper vaccines.
VPCRH AND/OR VPD (3.4.1)Efficacy: 95% (98% if 2 or more excess buffer)
This regulation for the member of the VPD is not only volunteered but extremely strictly, close military controlled therefore, we can assume reduce community contacts by 95% and 100% voluntary compliance. Saturation of VPDs and VPCRHs should be performed as described in chapter 2.8. With this, many more protective HI-generating ppl are available from the beginning, on the other hand, the not so old (i.e. AG1-2) age groups have a greater need for family and society.
VPHQ (3.4.2) Efficacy: 90% (95% if 2 or more excess buffer)
The regulation is mandatory and strictly personally controlled, we can assume to reduce the community contacts by 95% beside 95% obedience. The VPHQ have to stay at home and can walk outside strictly in the close neighborhood and they controlled and supplied by military staff. They are not allowed to use any transportation or not allowed to shop. The difference between VPHQ and the VPD is that both of them stay at home and the VPHQ can walk outside in the neighborhood or vicinity while the VPD can go to the district in a controlled manner. Therefore, the VP living in dense area preferable to be isolated especially in VPCRH or VPD, not in VPHQ.
VPHQSB (3.4.3.-6.) Efficacy: 70-75% (80% if 2x excess buffer, 85% if 3 or more excess buffer)
This is most recommended to consider for developing countries, when the VPD, VPCRH and VPHQ are not possible. They are also isolated in this NPI from the zero day. This is not the scheduled entry way. That (EM) HQSB related to the whole ppl of the certain AG (2.8.3.).
The regulation is mandatory and strictly personally controlled, we can assume to reduce the community contacts by 70-85% beside 70-85% obedience. MPs and/or police officers would also control them with digital devices for face recognition. Other criteria related them is identical with below detailed HQSB Protocol. To demonstrate also the effectiveness of this protocol the outcomes are evaluated in several values (70-75-80-85%) in the result. The results of the different efficacies are demonstrated in this section, which is acceptable even at 70%. The results suggest that this provides the most optimal, flexible, and least resource-intensive and highly adaptable, ubiquitous logistics with up to 85% efficiency.
The possibility of infection can be greatly reduced by the protocol of designated buses and shops in the following non-stop form:
- The most optimal solution is to run special buses (microbuses) on a special route, nonstop every day and keep shops open exclusively for the VP. This means running fewer buses and shops with signicantly less possibility of infection. The isolation of VP more effective than the with the time zone version. The most effective protocol is to use the dedicated buses and shops all day long.
- On buses, the driver and inspectors, MPs must already be protected, like all of the staff in the store as well. The interior is thoroughly disinfected by nights and ventilated continuously.
- VP have to move in small groups in clusters. On certain days and hours of the week, the same people should always move together, coordinated by an MP by cell phones, in the same path same time frame, so that the different clusters avoid each other. Even in the buses and shops, the clusters should keep the distance to each other as much as possible. Everybody should wear mask and avoiding face to face close talking.
- If infection occurs, the already demarcated number of cases increase the more effective contact tracing.
All public transport and supermarkets can be controlled simply and effortless with minimal human resources deployment of MP or police officer. The result and significance of these individual restrictions and they combination is that a dedicated age group can leave their home and walk outside in the close district in safe, where they live, but people cannot really go anywhere else, except by the bus controlled by the police officers.
In this manner, in practice, - that is related to the previous VPHQ protocol - the meetings of the elderly population are restricted only for relatives and grandchildren. However, with a purposeful, well-established, and determined communication, the government would make it clear to their relatives that the life of their loved elderly ones from now, principally depends only on them, during this pandemic period. If the necessary instructions or rules are not followed and the well-known necessary social distance and other hygiene practices (hand washing, wearing mask etc.) are not followed, safety cannot be maintained. Municipalities would provide additional supplies and home delivery (personal needs) that is not available in shops, except food. Ticketing or introducing other rules as described in chapter 2, is advisable in accordance with local custom conditions. If one or two old relative live in the same household other than the spouse, the same restriction applies to them. The feasibility problem of multigenerational households, dense districts, nursing homes is described in 2.7.3. and 2.7.4. Basically, they are advisable to isolate in VPCRH. (2.7.1.)
Among these versions the combination of AG1-3 in VPCRH, VPD or VPHQ (zero entry day) and the AG4 wil be in (EM)HQSB scheduled entry day, when the isolation of the considerable huge number of VP from the AG4 is not possible for the shortage of resources. (see: Rationale of the (EM)HQSB80+ in 3.8.3)
The HQSB+Age Group (AG) (e.g. HQSB55–69 or HQSB80+ etc) employs this NPIs, in a scheduled entry way. The “EM” always means a scheduled entry. That (EM)HQSB related to the whole population of the certain AG. The VP is not isolated in this case. They remain in the certain AGs.
The regulation should be mandatory in the course of this protocol. We can assume that the reduction in the number of contacts is 85% in community, as a result of 85% obedience and compliance of the implementation of the controlled mandatory regulation. In the basic HQSB scenario, we calculated 15% of outsider among the AG3 and/or AG4 population, who cannot or do not want to keep the rules, reducing the efficacy.
It is assumed that 15% of (EM)HQSB age groups (AG4 and optionally AG3) fail to be fully isolated from the virus or they ignore keeping the rules. In this way this part of the population increases proportionately the number of ppl and ICU/10k (identical to VP hereafter) in AG1-2 definitely, AG3 optionally) starting from the beginning (day 90) in the pre-entry period, as represented in Figure 2.9.3. and Table 2.9.3. The new ppl and ICU/10k [AGn]’ values for the corresponding groups are also modified according to averaging from the original ppl and ICU/10k [AGn] and the corresponding population.
If the scheduled entry of AG3 and AG4 takes place after the finally formed HI plateau, the (EM)HQBS can exert the maximal effect as it 85%. If the scheduled entry of AG3 and AG4 takes place earlier than the finally formed HI plateau, the (EM)HQBS shows lower efficiency and the mortality rate either from the remaining 85% of the group (plus the transferred 15%) is obviously equivalently higher, corresponding to the actual protective effect of the current HI.
The HQSB can deploy in addition to the ELSE EM model not only play a role as a scheduled entry group. However, it can also deploy in any ongoing outbreaks as a very effective prompt adaptive trigger mechanism if the actual epidemic parameters make it necessary any time at the appropriate locations over the appropriate time.
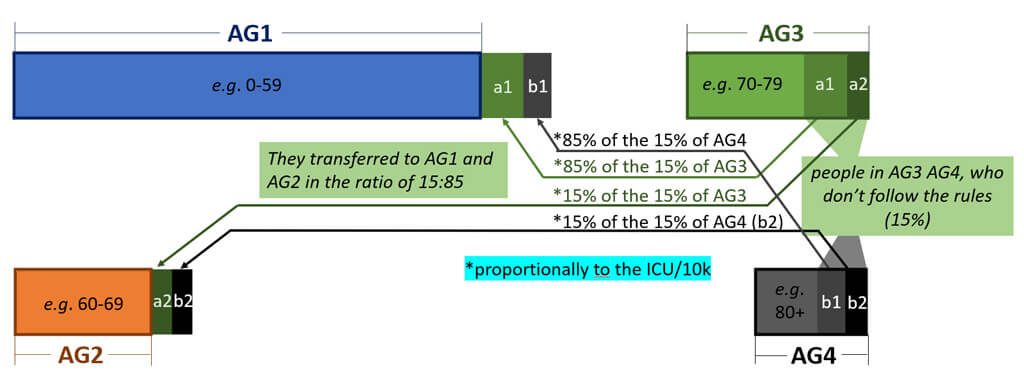
Figure 2.9.3. A schematic representation of the VP strategy, selecting the 15% of ppl and ICU/10k from the original elderly age groups of AG3, AG4 (in (EM)HQBS) and transferred them to the AG1 and AG2 in two subgroups in the ratio of 15:85. According to this model, the subgroup a1+a2 (from AG3) and b1+b2 (from AG4) are not fit to the restriction and thy mixed into the AG1 and AG2, respectively. The a1 and b1 are transferred to AG1, with limited restrictions and the absence of quarantine, while a2 and b2 are transferred to AG2 Table 2.9.3. If the AG3 not in (EM)HQBS but only the AG4, it is assumed that only 15% of AG4 fail to be fully isolated from the virus or they ignore keeping the rules, so this part of the population increases proportionally the number of ppl and ICU/10k (as VP) transferred to AG1-3.
Table 2.9.3. A dedicated example for the regrouping the 15% of the AG3 and AG4 to AG1 and AG2, distributing them into 15:85 ratio in the (EM)HQBS protocol, as demonstrated in accordance to Figure 2.9.3.
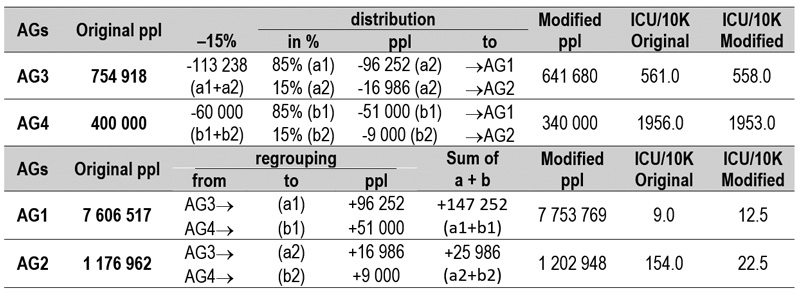
Table 2.9.4. Modified age group population and ICU/10k for AG1–4, when AG3 and AG4 is modified by VP strategy, as represented in Figure 2.7.3. The overall population is 9 938 392.

a100% = original; b100% excess buffer of VP; c200% of excess buffer of VP
As a brief conclusion, it is obvious that ELSE VP protocol (3.4) could significantly decrease the overall death rate in each of the age group according to the efficacy of the isolation of them, without the application of any other interventions, such as traditional NPI (2.9.1.).
Other NPIs can also significantly influence the development of the pandemic toward favorable directions and decrease the number of deaths or shorten the period. However, any combination of NPI and quarantine shift (scheduled entry) of AG3-4 will never reach the efficiency of ELSE VP protocol (3.4.).
In order to proof the supremacy of, the ELSE VP protocol (3.4.) over all the other possible models we present a few theoretical cases to illustrate that the ELSE VP protocol has the largest and most beneficial contribution to the reduction of the pandemic burden, in this section we examined and presenting two simplified studies of the pandemic. All cases discussed fitted for Hungary as a typically, small central European country with an easily comparable demographical statistics for the developed countries and easily comparable number (10 M) of the population. In our model, the pandemic starts in the 90th day in the year of 2020 (first day depicted the 31st March as zero day). This was the time, when the WHO declared the pandemic (28th of march), it correlates with the historical beginning of the natural outbreak of the COVID pandemic in Europe.
Study-1: Comparison of the Natural outbreak (Case-1), the NPI (Case-2) and ELSE protocol (Case-3)
In the first study, we compare the outcomes of the pandemic, the influence of the ICU bed (Case-1), the efficacy of the NPI (Case-2) under the Natural Outbreak model and the ELSE strategy (Case-3) in a short demonstration in Fig. 3.0.1. In the first case (Case-1), we are varying only the number of ICU bed (from 0 to an “unlimited” number of 25000) and NPI parameters (from 1 to 0 in the Control Panel and expressing in % in the text). The comparison of development of the Natural Outbreak pandemic curves, besides various ICU bed capacities (Fig. 3.0.1), undoubtedly proves that even an “unlimited” (>25 000 bed capacity) and extremely expensive health care system can only decrease the number of deaths by only 27% (19 755 reduction in number of death). Three examples are highlighted in the following section. The zero (0) bed represents the absence of health care capacity (Case-1a). The 2 500 beds (Case-1b) and 25 000 beds (Case-1c) model the normal default and the unlimited health care capacities, respectively. As a conclusion, we can state that increasing the bed capacity results only marginal benefit, as the number of deaths is reduced only by 27% despite an extreme health care budget. It should be emphasized that in all the calculated points, the developing HI values have reached a significant level (>65%). The developments of the pandemic for Case-1a and Case-1b, all the way to its completion, are represented in Figure 3.0.2 and 3.0.3.
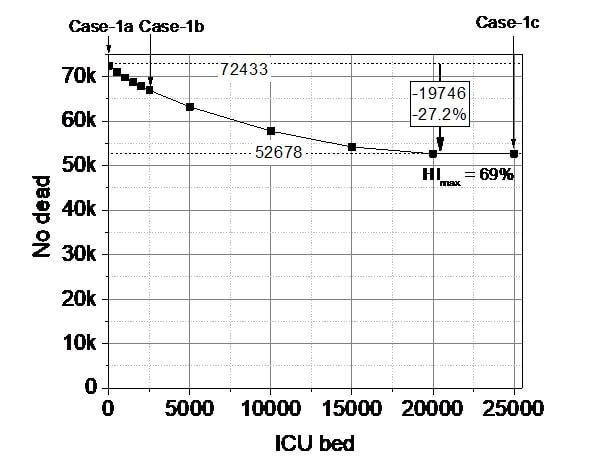
Figure 3.0.1. Left: Number of deaths depending on the number of available beds in intensive care ICU in the case of the Natural Outbreak (NOB) simulation.
Table 3.0.1. Summary of the preliminary results of Study-1, Case-1a–1c.
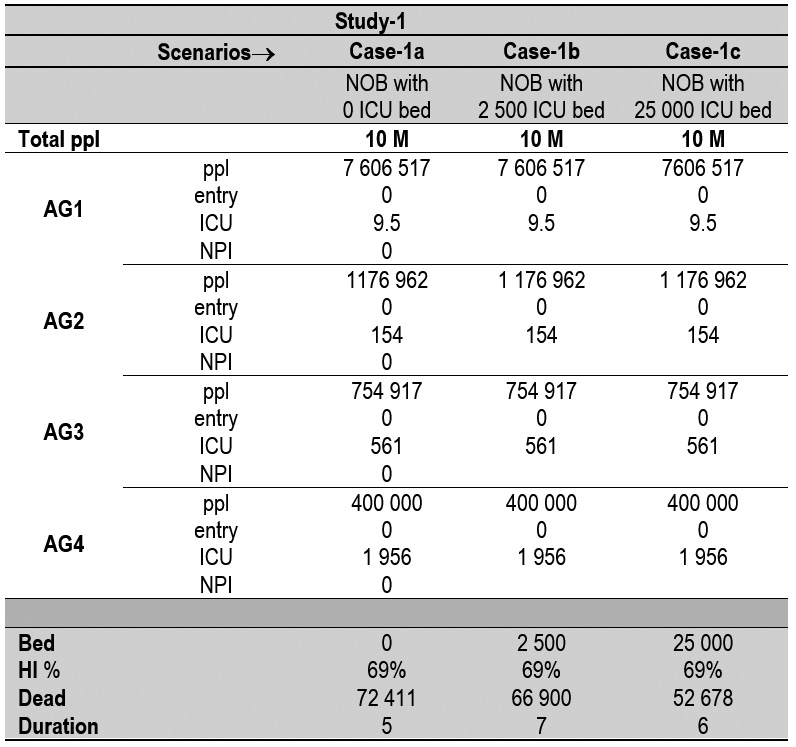
NOB = Natural OutBreak; ppl = population; AG = age group; ICU = intensive care unit.
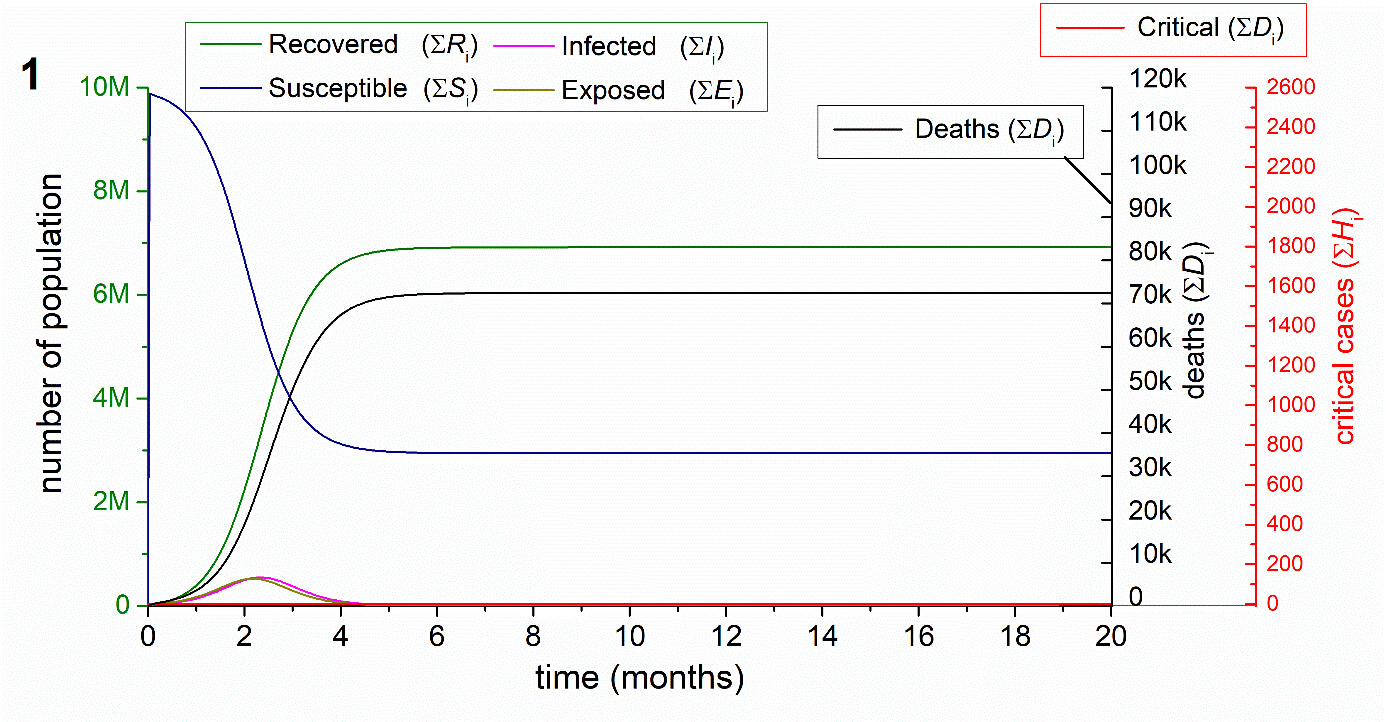
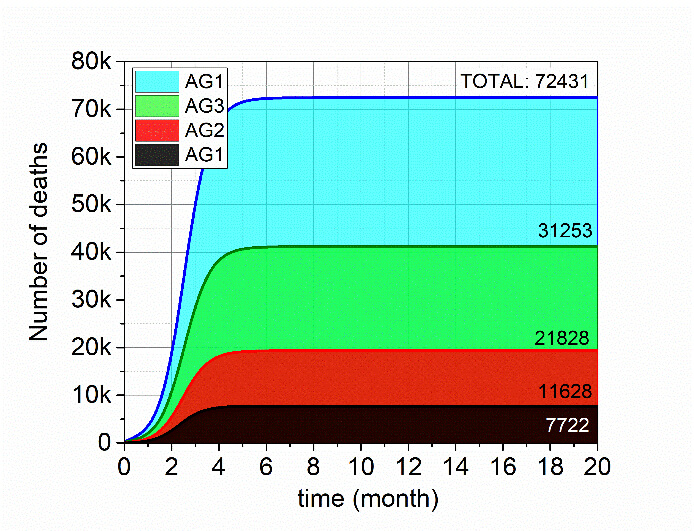

Figure 3.0.2. A. Case-1a study, the Natural Outbreak without ICU bed. The upper graph represents the development of pandemic as the function of time (month). The graph at the lower line left-hand side shows the number of deaths in various (AG) as the function of time. The bar diagram at the lower line, the right-hand side shows the distribution of the number of deaths between the four age groups (AG) in absolute value and in percentage (%).



Figure 3.0.3. Case-1b study, the Natural Outbreak with 2500 ICU bed. The upper graph represents the development of pandemic as the function of time (month). The graph at the lower line left-hand side shows the number of deaths in various (AG) as the function of time. The bar diagram at the lower, the right-hand side shows the distribution of the number of deaths between the four age groups (AG) in absolute value and in percentage (%).
An alternate pandemic management, which is often mentioned in the media, is the application of NPI protocol (Case-2). In Case-2, we modelled the outcome of the Natural Outbreak pandemic scenarios, with various NPIs (0%, 20%, 40%, 60% 100%), as Fig. 3.0.4 represents. As it is obvious, the high protection of NPI produce a dramatic drop in the number of deaths, irrespectively to the number of beds. However, under high protection (NPI is larger than 40%), the herd immunity (HI) has no chance to develop to the desired value (>58%). It means, that after releasing the restrictions, the rate of the pandemic will return to its original level. Consequently, in most of these cases, the application of any NPI or their combinations, ranging from 20% to 100%, will only postpone the dramatic outcome
These results allow us to conclude that NPI protocol although can pause the pandemic, but the application of NPI protocol cannot terminate the pandemic except an theoretical totality wartime-like curfew for three weeks all over the word at a same time. Any loosening in the NPI regulation, after the mitigation of the curves, the infection will restart again. It only shifts the rest of the scenario and the peaks, leading to a mostly overwhelmed ICU related segments of the health care system.
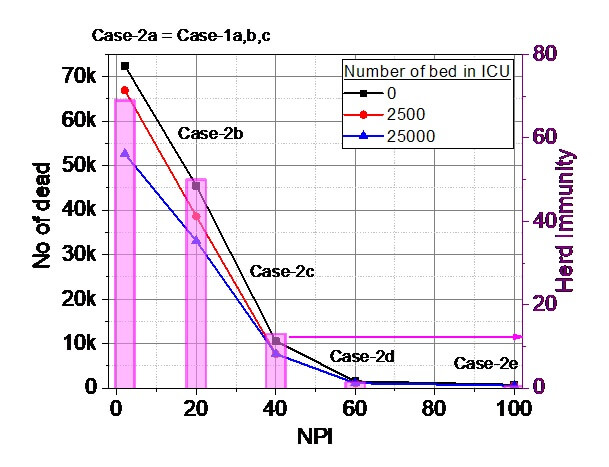
Figure 3.0.4. Case-2. Number of deaths depending on the NPI in the case of the Natural Outbreak simulation, considering three scenarios for the number of available beds in intensive care (0 – black; 2 500 – red; 25 000 - blue). Purple bar (right axis) illustrates the developing herd immunities (HI) (in %) for the three cases. The other parameters are set as default.
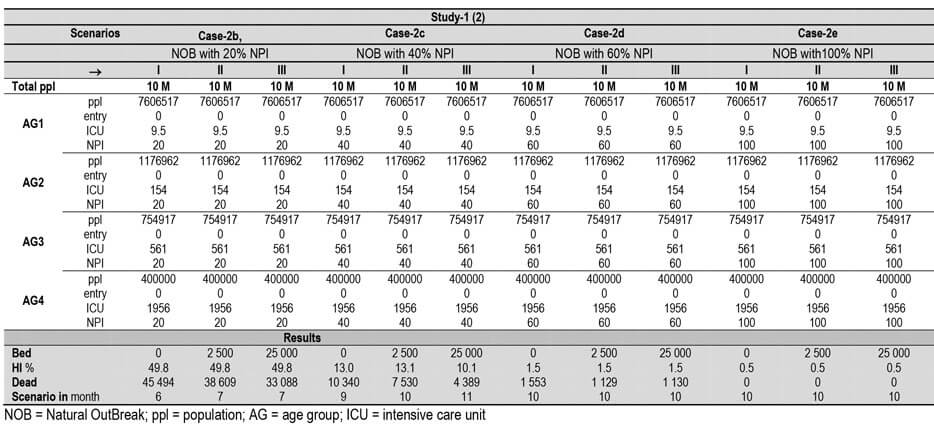
The third alternative is our ELSE strategy. In the first turn (Case-3), a simplified ELSE-1 protocol was used, in order to give a more understandable conclusion presented in this section. ELSE-1 protocol splits the entire population into four age groups (AG1–AG4). Here, AG1 and AG2 are exposed to the infection from the 0th day. The AG3 and AG4 groups are allowed to return into the population after a defined shifted period (X = 0–260 days), as shown in Fig. 3.0.5 Rigth. The results are summarized in Fig. 3. 0.5 Left, and it clearly shows, that the prolongation of the entry date X results dramatic decrease in the number of deaths, almost irrespectively to the bed capacity. The maximum quarantine shift results 80% reduction. Moreover, it is more pronounced that at 150-day (5 months) shift, the number of deaths is already almost independent from the number of ICU beds, predicting less of a burden for the health care system. It is more important that, at all the points in Fig. 3.0.5, the developing HI values have reached a significant level (>54%). This result allows us to conclude that the ELSE-1 strategy can terminate the pandemic, without the chance to restart. The development of the pandemic is represented by two selected examples, these are the X= 60 days (Case-3a) and X = 90-day quarantine shifts (Case-3b) in Fig. 3.0.6. and 3.0.7.

Figure 3.0.5. Left: Summary of the Case-3 study (ELSE-1). Number of deaths depending on the quarantine shift (X in days) for three examples of the number of available beds in intensive care (0 – black; 2500 – red; 25000 - green). The developing herd immunities for the points are represented by purple bars (calibration is on the right axes). Right: The quarantine system of the ELSE-1 model for the Case-3 study.
Table 3.0.3a. Summary of the preliminary results of Study-1 (ELSE-1), Case-3.

Table 3.0.3b. Summary of the preliminary results of Study-1 (ELSE-1), Case-3, continued.
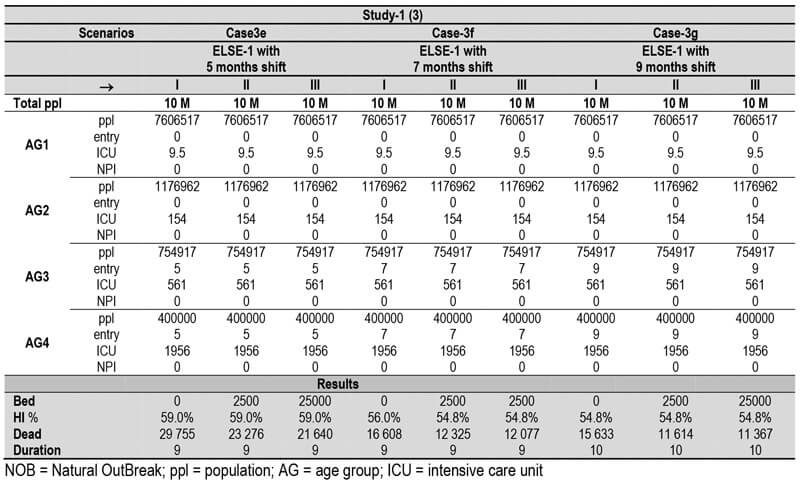


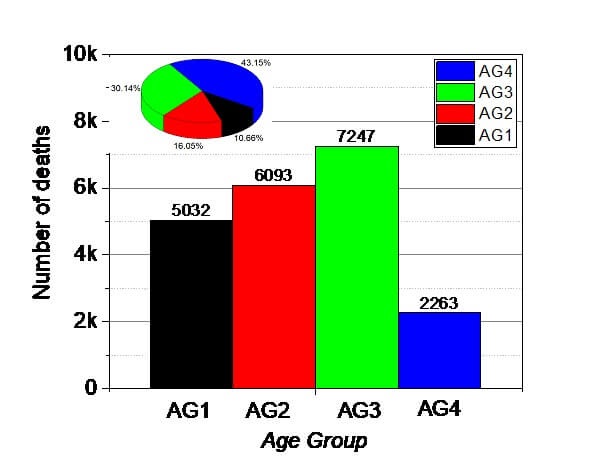
Figure 3.0.6. Case-3a study, the ELSE-1 protocol with 60 days of quarantine period. The upper graph represents the development of pandemic as the function of time (month). The graph at the lower line left-hand side shows the number of deaths in various (AG) as the function of time. The bar diagram at the lower, the right-hand side shows the distribution of the number of deaths between the four age groups (AG) in absolute value and in percentage (%).



Figure 3.0.7. Case-3b study, the ELSE-1 strategy with 90 days of quarantine period. The upper graph represents the development of pandemic as the function of time (month). The graph at the lower line left-hand side shows the number of deaths in various (AG) as the function of time. The bar diagram at the lower, the right-hand side shows the distribution of the number of deaths between the four age groups (AG) in absolute value and in percentage (%).
Study-2: Analysis of the Natural Outbreak (Case-1) and sophisticated ELSE-2 protocol (Case-4)
In the next paragraph, we compare and analyze four selected pandemic situations. The first two cases represent again the Natural Outbreak with zero ICU bed (0 bed, in Case-1a) and with a typical number of ICU beds (2500 beds, in Case-1b). Case-4 and Case-5 correspond to the extended ELSE-2 protocol, where AG2, AG3 and AG4 groups are allowed to enter sequentially into the society after a defined shifted period (shift = X, 2X and 3X for AG1, AG2 andAG3 respectively). The period shifts are X= 60 (Case-4a) and X= 90 days (Case-4b), respectively, as showed in Fig. 3.0.8.
The left-hand side graph in Fig. 3.0.9 summarize the outcomes of the four cases. It clearly represents the beneficial effect of the ELSE-2 protocol in the reduction of the number of deaths. The number of deaths decreases in all the four age groups (AG1–4), especially in AG3 and AG4, in a sharp contrast with Case-1. This is due to the effect of ELSE-2 protocol exclusively. We would like to emphasize that the number of deaths is also decreasing in AG1 and AG2 for Cases-4a and 4b, compared to the Natural outbreak Cases-1a and 1b. This effect can be attributed to the limited contact number in Case-4a and 4b at the beginning of the pandemic. This observation an ultimate proof that ELSE-2 is the most effective strategy, which must always be the priority method in pandemic interventions. It should be mentioned, that the pandemic period is elongated to 9-11 months for ELSE-2, instead of the original predicted 5 month long pandemic period for the Natural Outbreak.

Figure 3.0.8. The quarantine system of the ELSE-2 protocol for the Cases 4, given in months.

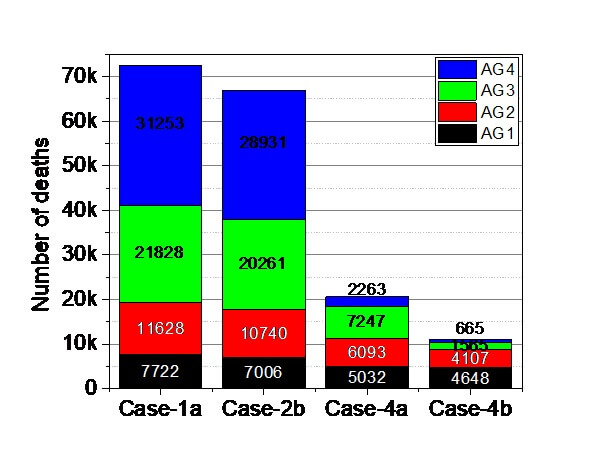
Figure 3.0.9. Left: The beneficial effect of ELSE-2 protocol (Case-4a, Case-4b), including the sequential entries of AG1–AG4 (green), compared to the two cases of the Natural Outbreak with 0 bed (black, Case-1a) and 2 500 bed (red, Case-1b). Right: The sum of predicted causalities at the end of the pandemic with the representation of the four age groups. The pandemic period is 5 months for Nat Outbreak, while it is elongated to 11 months for ELSE.
Table 3.0.4. Summary of the preliminary results of ELSE-2.

ppl = population; AG = age group; ICU = intensive care unit
As a conclusion, it is obvious that both ELSE protocols (ELSE-1 and 2) could significantly decrease the overall death rate without the application of any other interventions (such as NPI), besides a tolerable elongation of the duration. ELSE protocols could decrease the death counts in each of the age group as well, but the most dramatic decrease can be obtained in AG3 and AG4.
Other NPIs can also significantly influence the development of the pandemic toward favorable directions and decrease the number of deaths or shorten the period. However, any individual NPI or any combination of them will never reach the efficiency of ELSE protocols.
In the first section of the detailed results the natural outbreak was modelled, excluding any interventions. In this case the four age groups (AG1–4) were released at the same time (90. day) without having bed capacity in the intensive care. We set the standard parameters, as listed before. This scenario represents the standard and most negative point to compare the effect of all the suggested scenarios.
As the result of the of the pandemic process without restriction and ICU bed capacity, we have experienced a high herd immunity (HI = 69%), besides a significant number of fatalities = 72.4K (IFR = 0.9%). The pandemic situation, however, finished within 5 months




In the next step, we studied the natural outbreak situation, with – hypothetically - limitless ICU bed capacity for serious cases (25 000 bed). The four age groups (AG1–4) were released also at the same time (90. day), beside the standard parameters. This scenario provides information about the situation, when the health care capacity has no limit. The excess number of deaths, comparing the real ICU beds protected lives.
The result of the of the pandemic process in this case reaches a high herd immunity value (HI = 69%), with a smaller number of fatalities = 52.6K (IFR = 0.9%) and it finished within rapidly 6 months. This case proves that the extended health care capacity itself does not serve the sufficient protection for the society. Most of the fatalities comes from AG4 and AG3, so the elderly population cannot be defended without the use of different NPI and/or isolation (see 3.2).
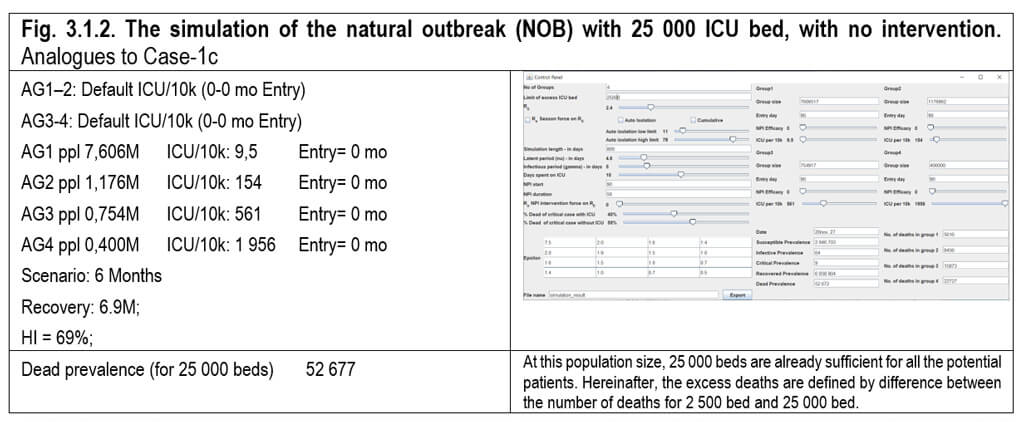



In this paragraph, we studied the natural outbreak situation, with a rational 2 500 ICU bed capacity/10M for serious cases (2.5/10k). (2.8.) This 2 500 ICU bed is representative at this country size, called as real number of beds. The four age groups (AG1–4) were released at the same time (0th day), beside the standard parameters. This scenario represents a typical situation, happened in most of the countries at the beginning of the pandemic. In this case, the result of the of the pandemic process reaches a high herd immunity value (HI = 69%), with less number of fatalities = 66.9K (IFR = 0.9%) and it finished within rapidly 6 months. The reduced number of the deaths due to the 2 500 beds, saving only 5 500 lives, which is only 7.5% of decrease.

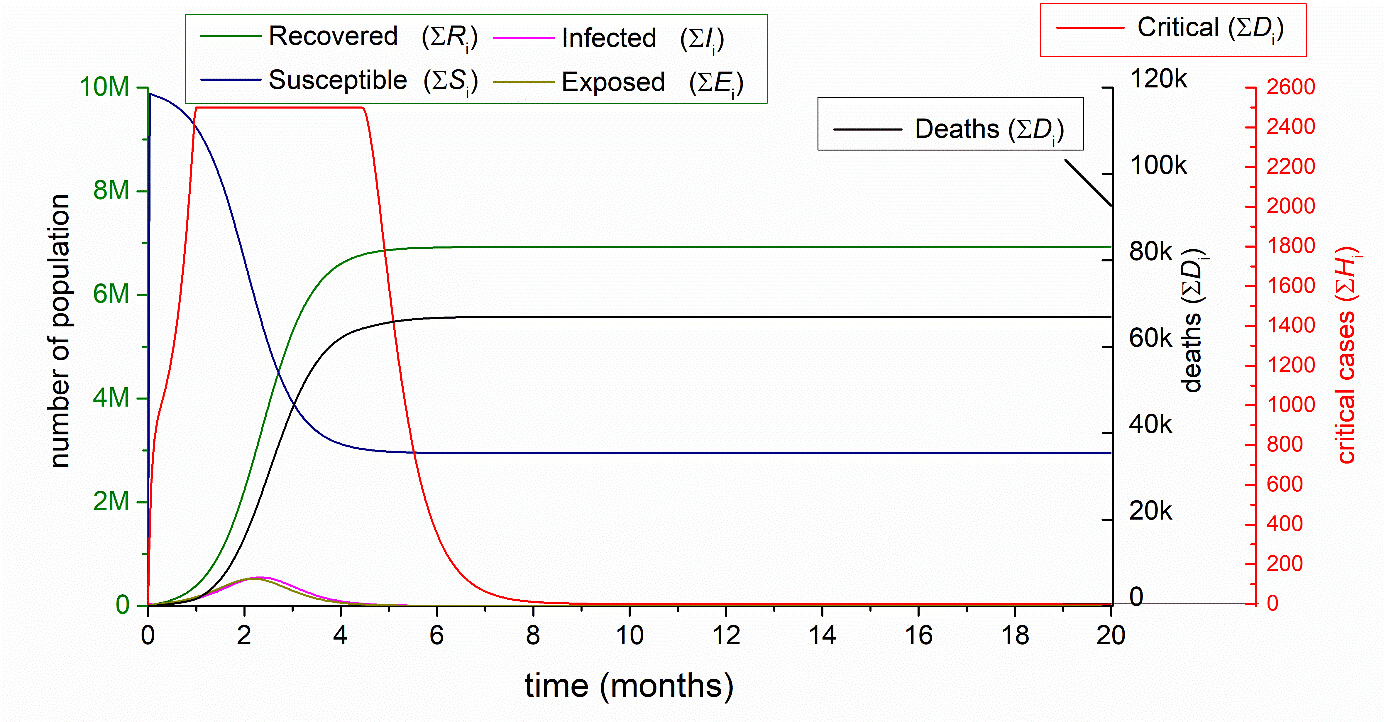
Here, we studied the effect of the season force (40% reducing of the R0=2,4 Re=1.44) – adapted from Kissler et al.{*} in the case of the natural outbreak situation, with a rational 2500 ICU bed capacity for serious cases (2.5/10k). The four age groups (AG1–4) were released at the same time (0th day), beside the standard parameters. In this case, the result of the of the pandemic process reaches a high herd immunity value (HI = 45%), with a smaller number of fatalities = 32.3K and it finished within 15 months. The reduced number of the deaths due to the lower Re value during the summer. This scenario has already been refuted by several findings, namely the summer had no significant attenuation effect on the pandemic.


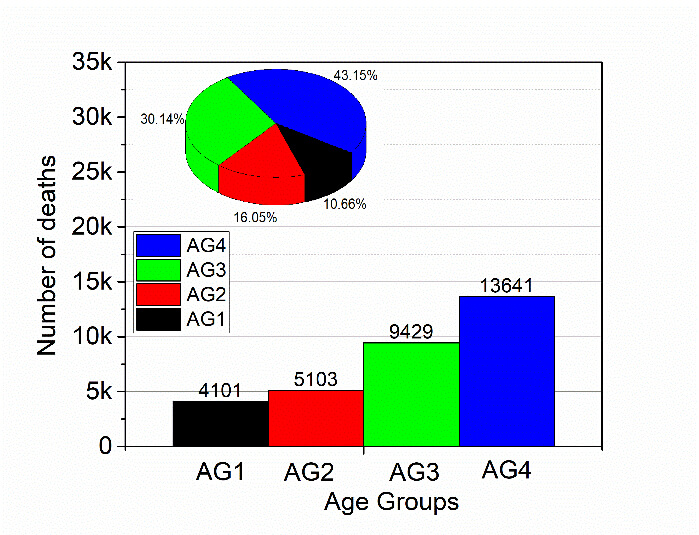
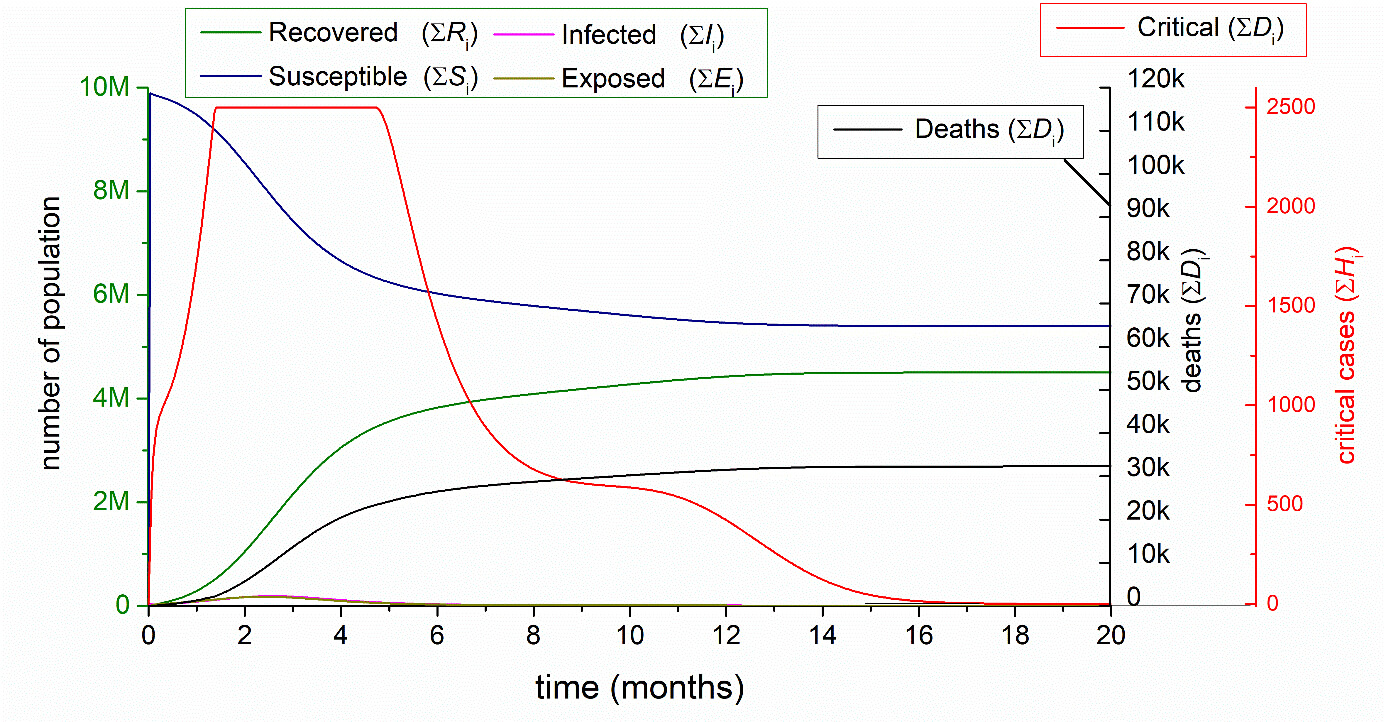
We studied the situation, when only AG1 and AG2 are entered into the pandemic, while AG3 and AG4 are “closed forever in quarantine”. This scenario includes a rational 2 500 ICU bed capacity for serious cases (2.5/10k). The two age groups (AG1–2) were released at the same time (0th day), beside the standard parameters. In this case, the number of fatalities = 10.5K and it finished within 6 months.
With this model, we want to demonstrate that up to 10K people will die from AG1-AG2 among the potential 25K VPs (7K in AG1 + 18K in AG2). This is important for the argument that how many deaths is resulted by the younger generations.




The most important conclusion of this section (Table 3.1.6.1 and Figure 3.1.6.1) is that even if unlimited numbers of ICU beds are available, the number of deaths decreased moderately (–27%). There is no point to invest exclusively into the number of ICU bed capacities in the health care system, which is the last step of the possible tools of the interventions. We have proven that the optimal situation can be reached only by the combination of the multistep interventions that creates together the highest HI as early as possible. Many studies also agreed that HI is the most important protective factor in the long term.
Table 3.1.6.1. Summary of the five Natural outbreak studies. Entry is given in months.
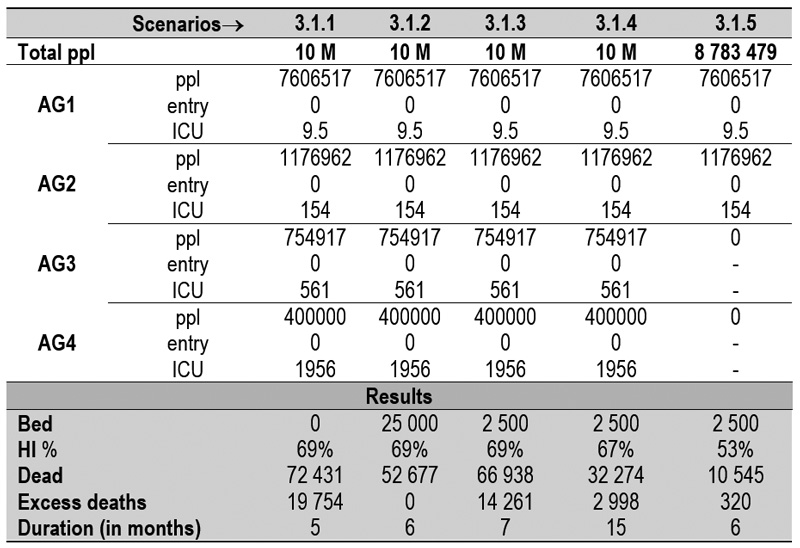
ppl = population; AG = age group; ICU = intensive care unit

Fig. 3.1.6.1. Comparison of the five Natural Outbreak cases presented previously in chapter 3.1.1.– 3.1.5.
In this section, we elaborated in a study, where AG1 and AG2 enter at 0th day, but the entry days of AG3 and AG4 are shifted in five steps by 30 days, in each steps, without any NPI (0%). This EM model illustrates the 1st quarantine method (see Fig. 3.2.6). AG1–4 is set in default parameters. The 100 % efficacy refers to the theoretical 100% protection for equally for each AG. The following figures (Fig. 3.2.1–3.2.5) show the consequences of the shift of the entry days of AG3 and AG4. If we compare these figures, they show that the later we leave the AG3 and AG3 to enter, the lower the number of the deaths occur. The numerical comparisons are shown in the final table (Table 3.2.1) together with the graphical representation in the last figure (Fig. 3.2.6).

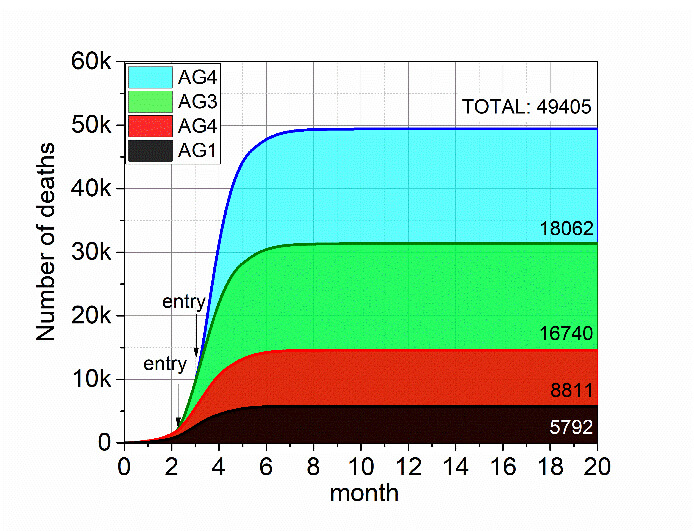

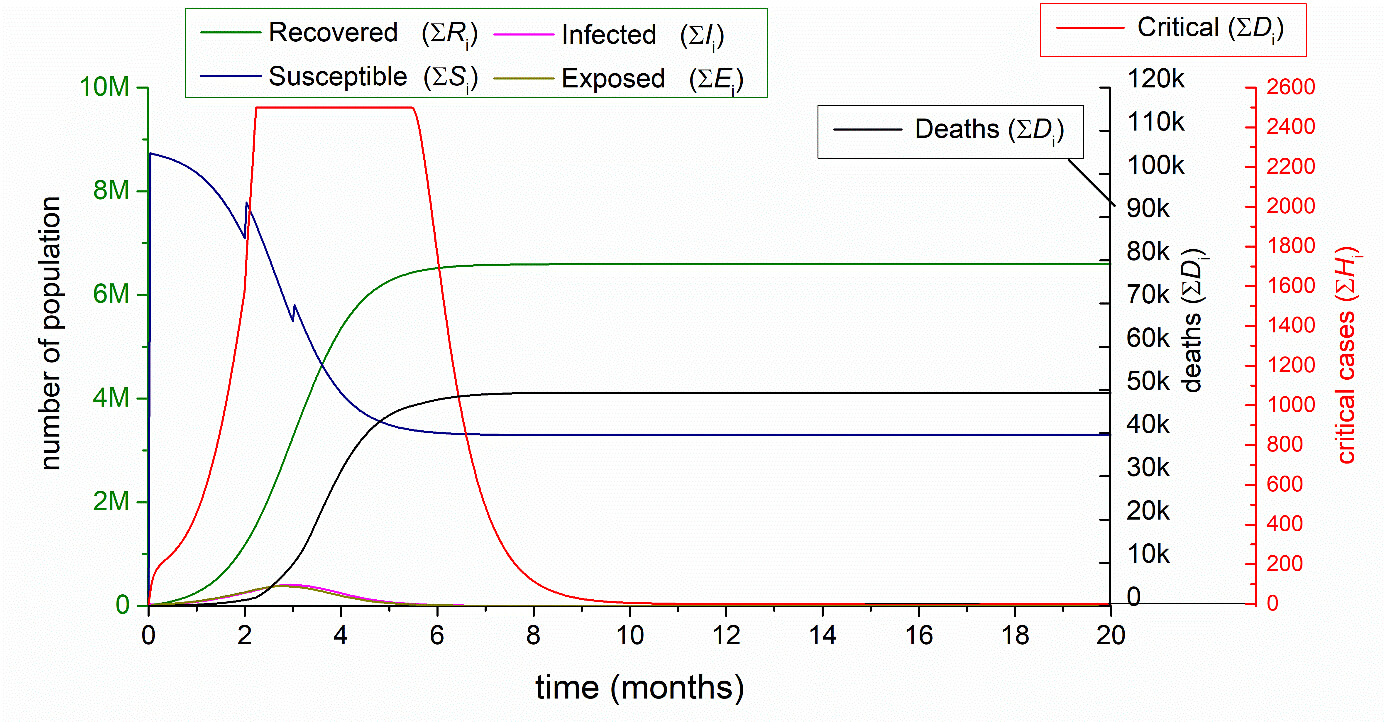





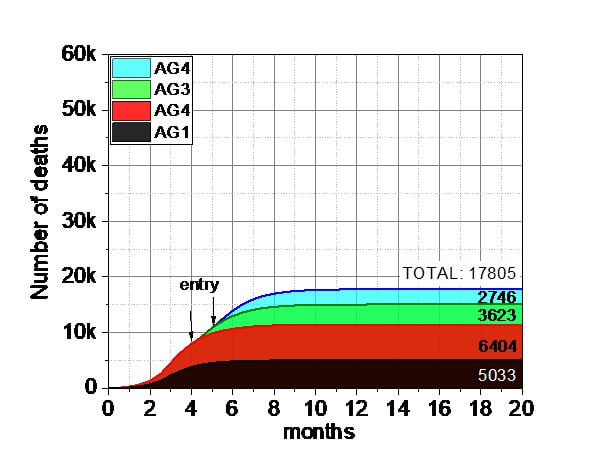


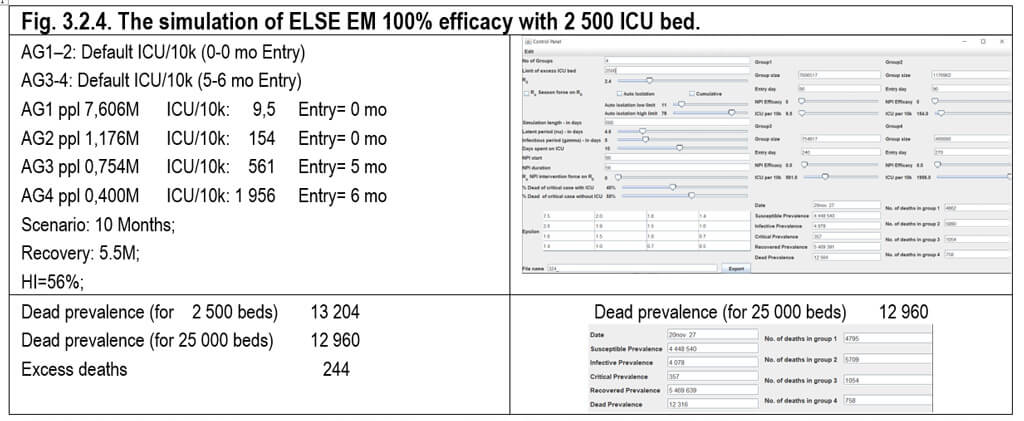
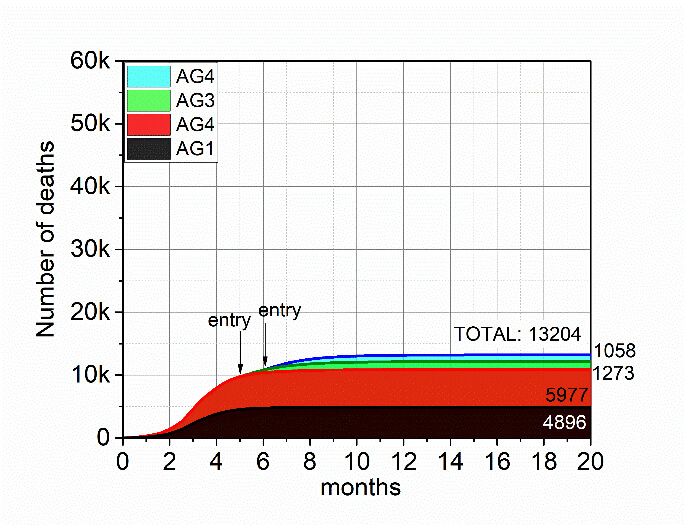

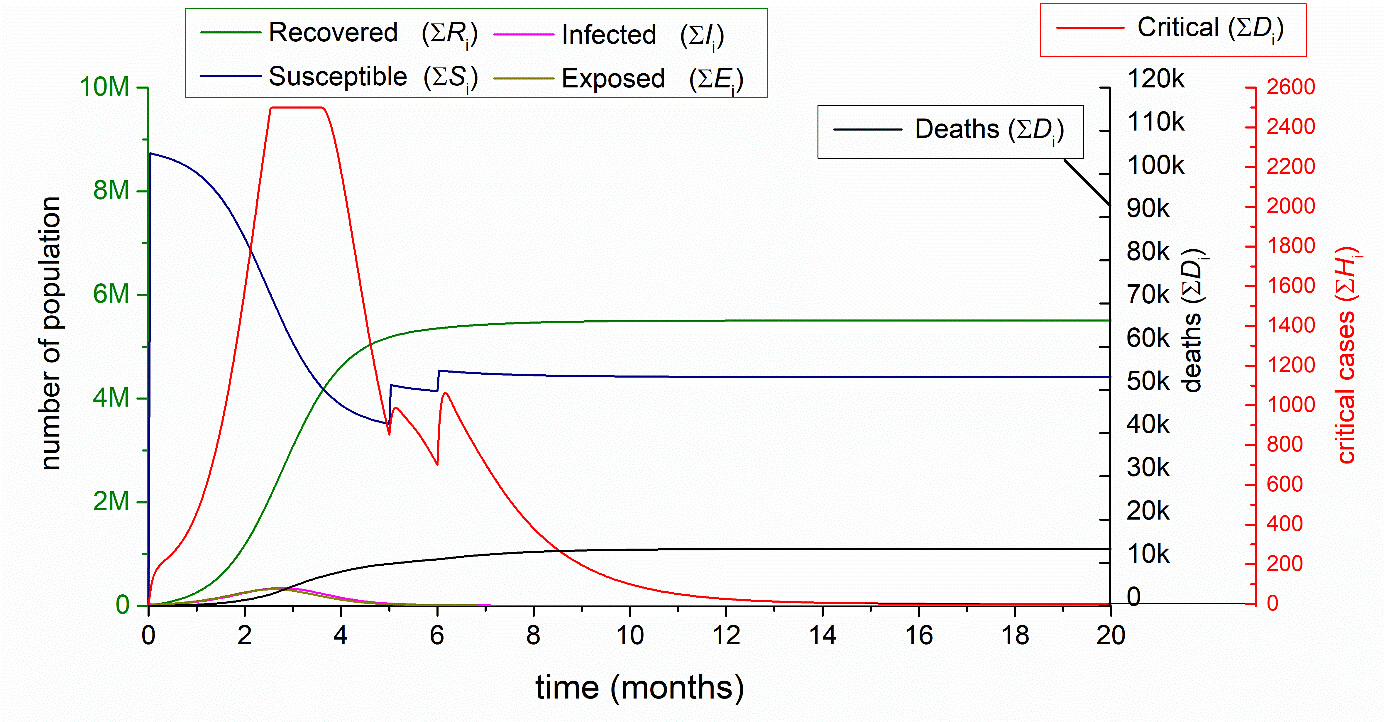



Table 3.2.1. Summary of the five ELSE EM 100% efficacy cases 3.2.1–3.2.5 in comparison with 3.1.3 (Nat Outbreak NOB with 2 500 beds remaining 85%, AG1-4 0-0-0-0 mo Entry). In 3.2.1-3.2.5 the AG1-2 tranferred 15% t ICU/10k (0-0 mo Entry) from AG 3-4 EM Default ICU/10k (2-3 mo, 3-4 mo, 4-5 mo, 5-6 mo, 6-7mo Entry) 100% Efficacy (The 100 % efficacy refers to the theoretical 100% protection for AG3-4.).
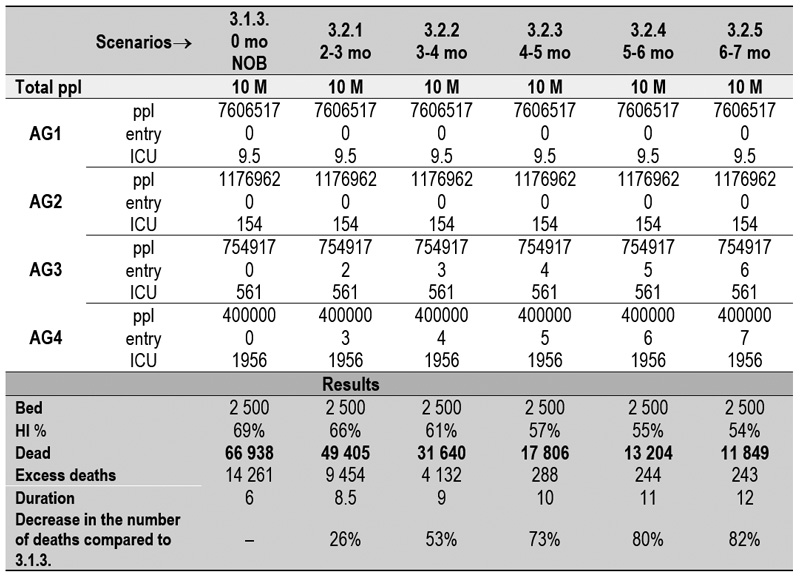
ppl = population; AG = age group; ICU = intensive care unit
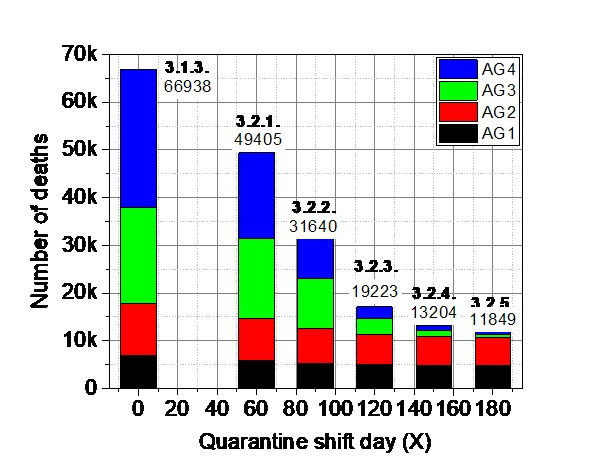
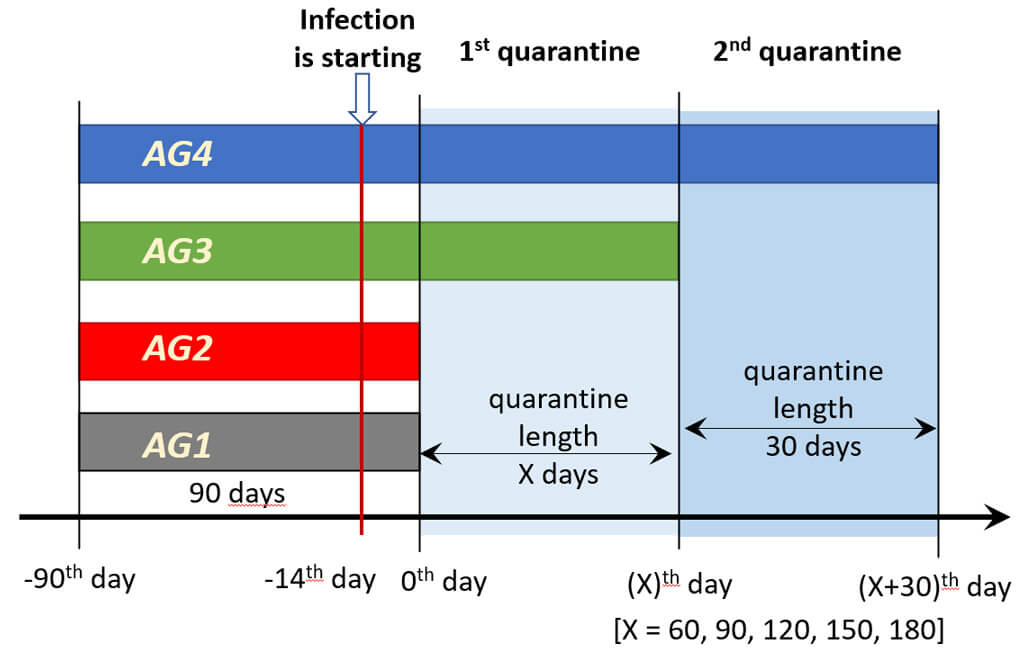
Fig. 3. 2. 6. Left: Summary of the ELSE EM 100% efficacy, applying the 1st quarantine method (for 2nd quarantine method see section 3.3). and represented by Cases 3.2.1–3.2.5 in comparison with 3.1.3. (Natural outbreak with 2 500 ICU beds). Right: The 1st quarantine model, which is applied in chapter 3.2. Comparing the results of Fig. 3.2.1–3.2.5, one may conclude that a longer quarantine period – as the entry reaches the plateau of the developed Herd Immunity - finally leads a decreased number of deaths. After the quarantine shift of 4 mo the number of deaths decreased below 20 000. At 6 mo, it close to 10 000. However, not only the sum of the number of deaths decreased, but the individual age-groups also exhibit lower numbers, which one of the ultimate benefits of the ELSE. Besides these advantages, the duration of the pandemic is elongated somewhat, but in an optimal choice, it may terminate within a year. The non-restricted populations in AG1 and AG2 however will continue the normal work.
In the next section, continued the ELSE-EM study was continued, in which only AG1 enters at 0th day, but the entry days of AG2, AG3 and AG4 are varied systematically in each step (2nd quarantine methods). The model also excludes the NPI (0%). AG1–AG4 is set according to the parameters of Table and Fig. 2.9.2.1.


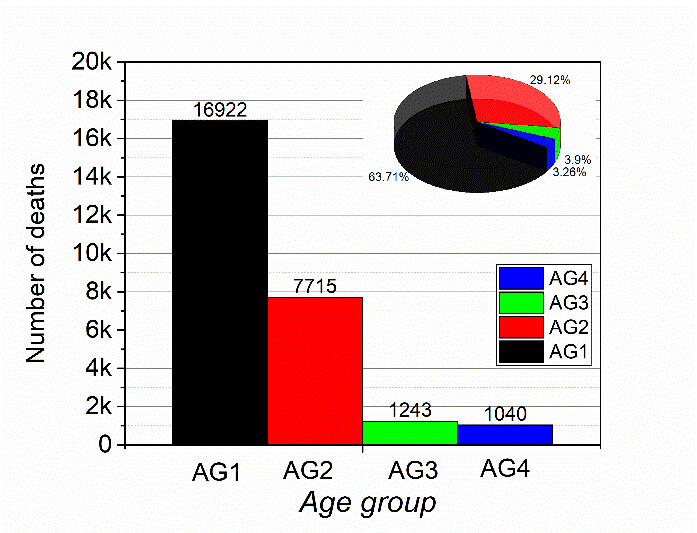
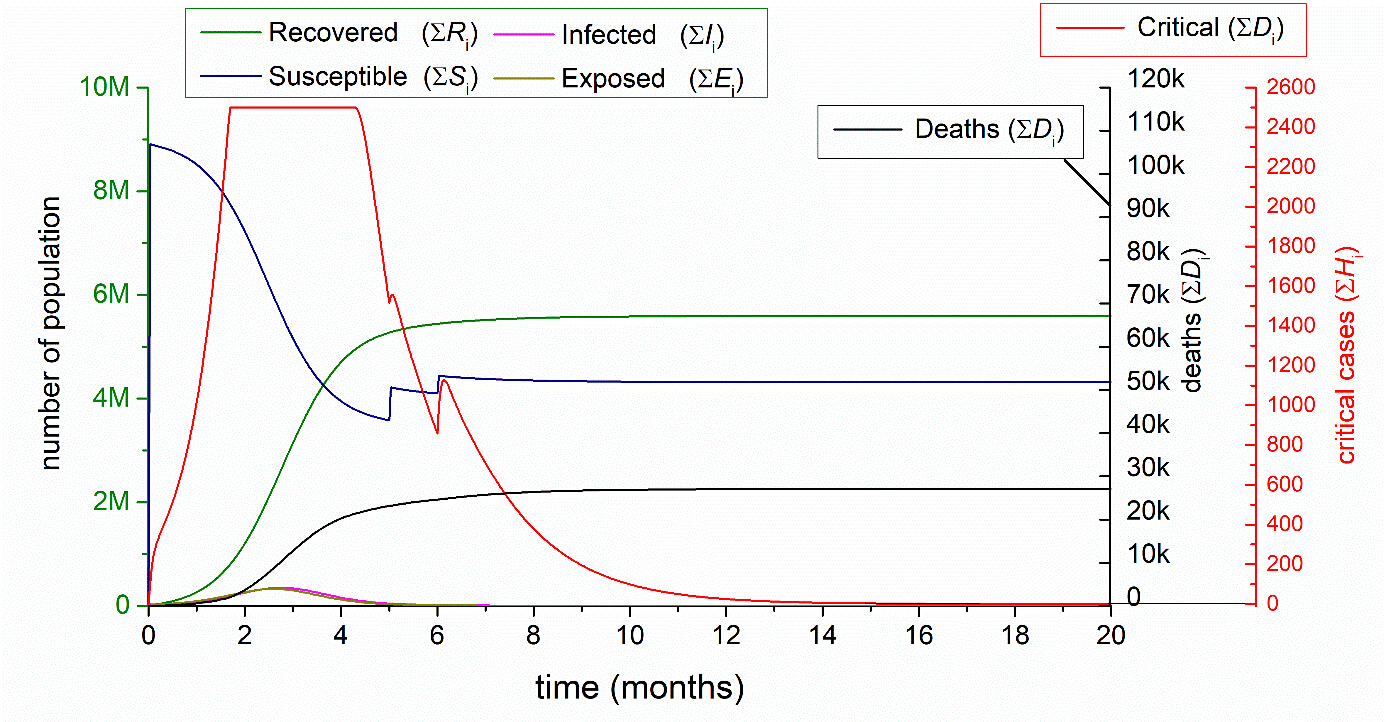

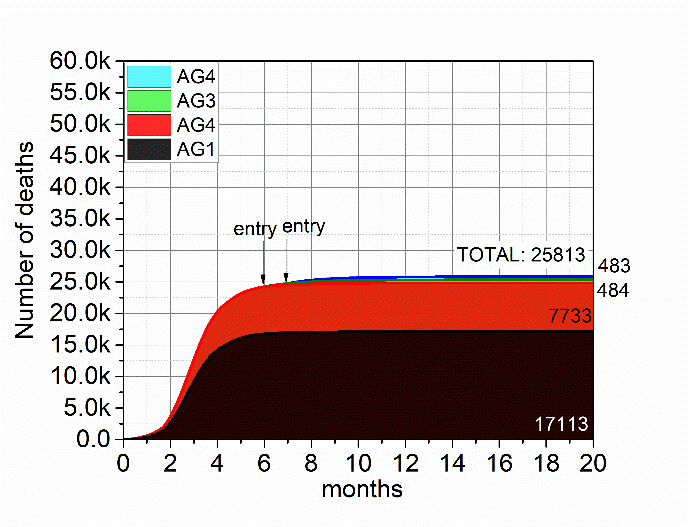

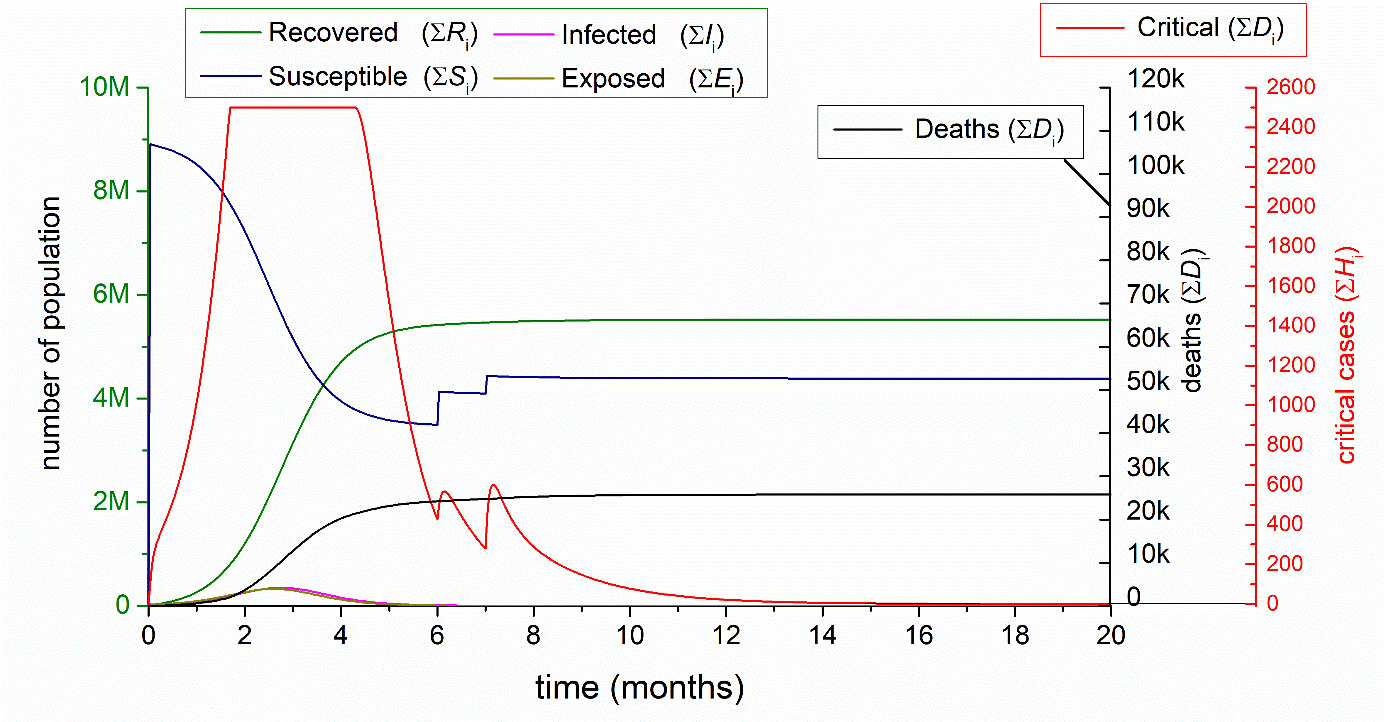
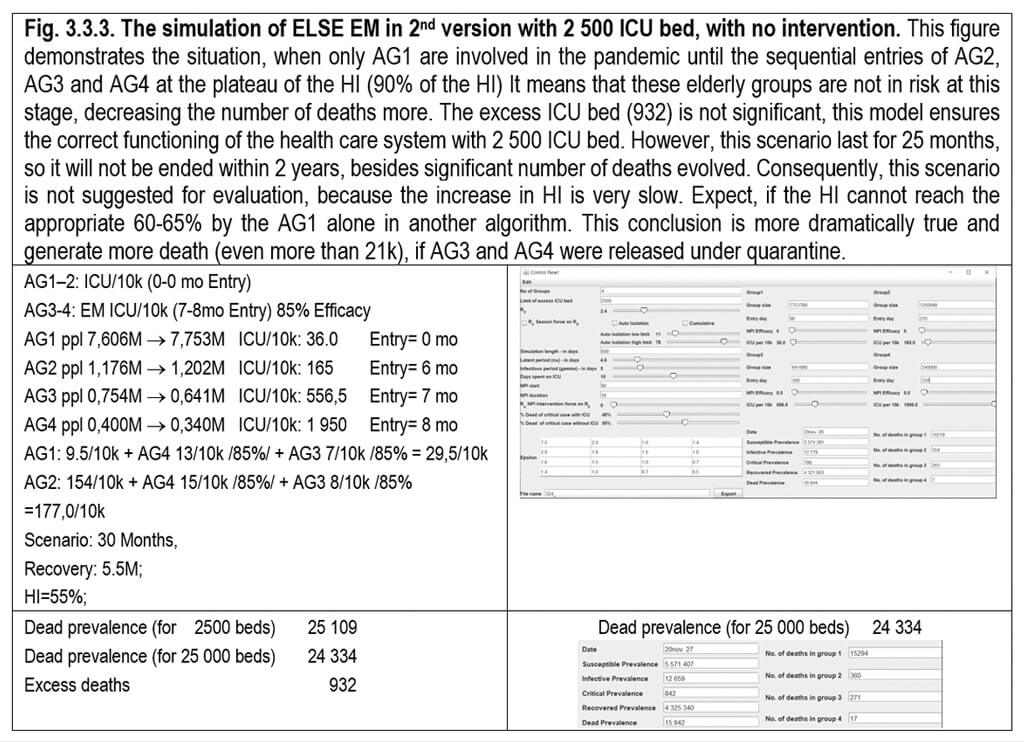
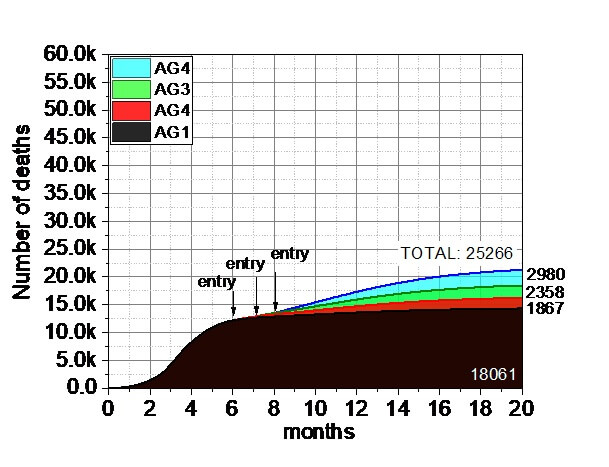
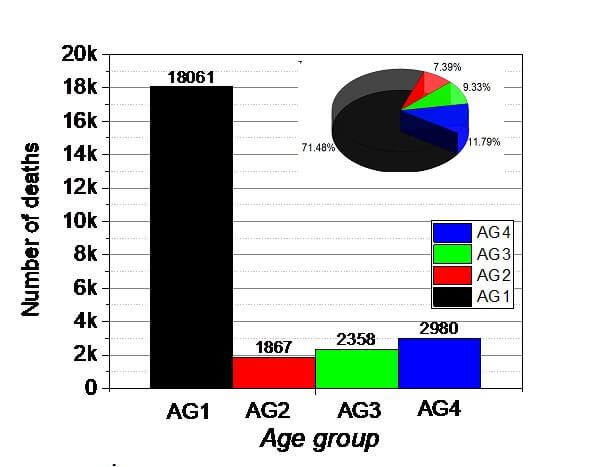

Table 3.3.1. Summary of the ELSE EM 85% efficacy cases 3.3.1–3.3.3. in comparison with 3.1.3 (Nat Outbreak NOB with 2 500 beds, AG1-4 0-0-0-0 mo Entry). In 3.3.1-3.3.2. the AG1-2 transferred 15% ICU/10k from AG3-4 (0-0 mo Entry) AG 3-4 EM remained 85% ICU/10k (5-6 mo, 6-7 mo Entry) 85% Efficacy. In 3.3.3. the AG1 transferred 15% ICU/10k from AG2-3-4 (0 mo Entry) AG 2-3-4 EM remained 85% ICU/10k (6-7-8mo Entry) 85% Efficacy (The 85 % efficacy refers to the theoretical 85% protection for AG3-4) and AG2-3-4 respectively. Summary table of the three scenarios in 3.3, simulating the ELSE EM protocol with 2nd quarantine model. 85%.


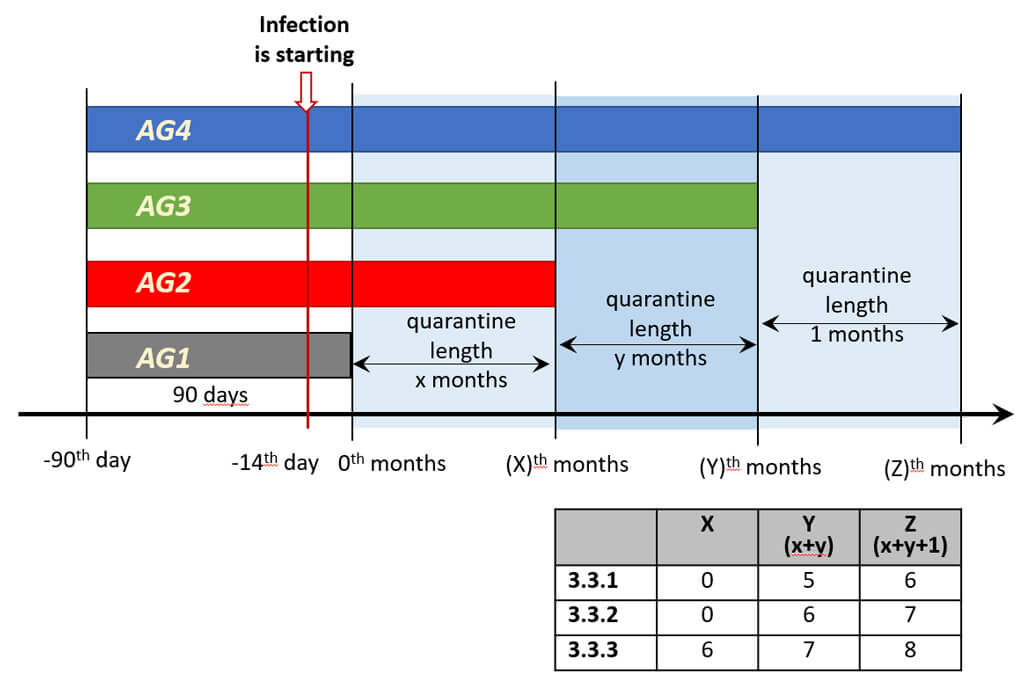
Fig. 3.3.4. Left: Summary of the five ELSE EM cases 3.3.1–3.3.3 in comparison with 3.1.3. Right: The 2nd quarantine model, applied in chapter 3.3. The 2st quarantine version is detailed in the Figure Comparing the results of Fig. 3.2.6–3.3.4, one may conclude that a longer quarantine period finally leads a decreased number of deaths. In this frame, the optimal choice of the quarantine shift may be in between day 120 (4 mo) and 150 days (5 mo), which decrease the number of deaths below 30 000. However, not only the sum of the number of deaths decreased, but the individual age-groups also exhibit lower numbers, which one of the ultimate benefits of the ELSE. Besides that, the duration of the pandemic is elongated somewhat, but in an optimal choice, it may terminate within a year. The non-restricted populations in AG1 and AG2, however will continue the normal work, keeping the economy near to the normal level. In a relative context, the number of deaths in AG1 possess significantly larger percent death, because many of them of the subpopulation (15% ppl. incl. 15% corresponding VP) from AG3 and AG4 are transferred ti AG1 and AG2. Overall conclusion is that the Isolation of VP absolutely important.(3.4.)
The Vulnerable Population (VP) Protocol for the VP members described in 2.9.2. The systematic examples below represent the effect of the VP protocol under VPCRH/VPD (95%), VPHQ (90%) and VPHQSB (85%-70%) control. The efficacy decreases from 95% to 70%. As the final Table 3.4.1 and Figure 3.4.6 conclude that the VP 95% efficacy can decrease the number of deaths dramatically (66 953 ® 4 020). Even, the 70% efficacy may result 18 621 number deaths, which corresponds to the saving of ca 70% of the VP. However, this means a very rigid military system, in case of VPCRH during the transport time to the cruisers resorts, in VPD continuously with maximal number, in VPHQ the less military burden. With VPHQBS similar like VPD IN 80-85% efficacy with very severe dealings, but with 70-75% efficacy with lower obedience and less controlled.
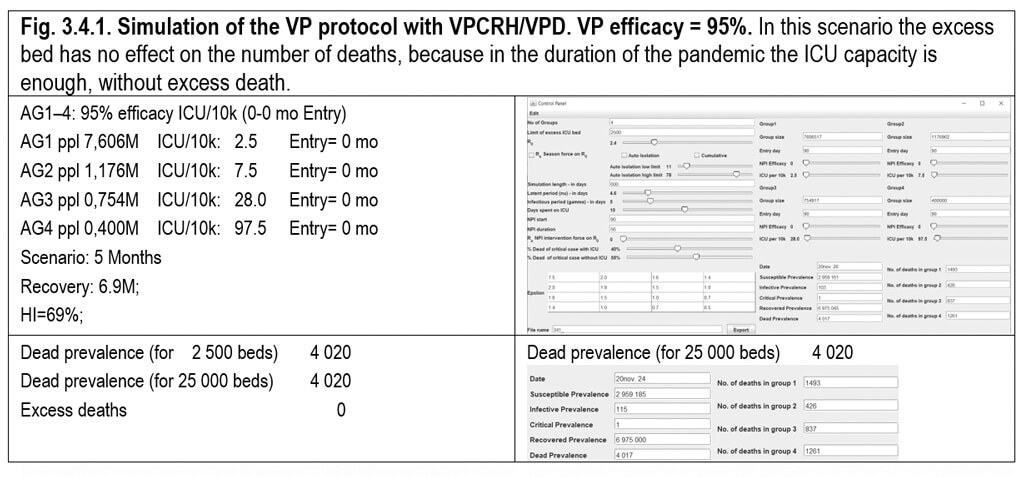


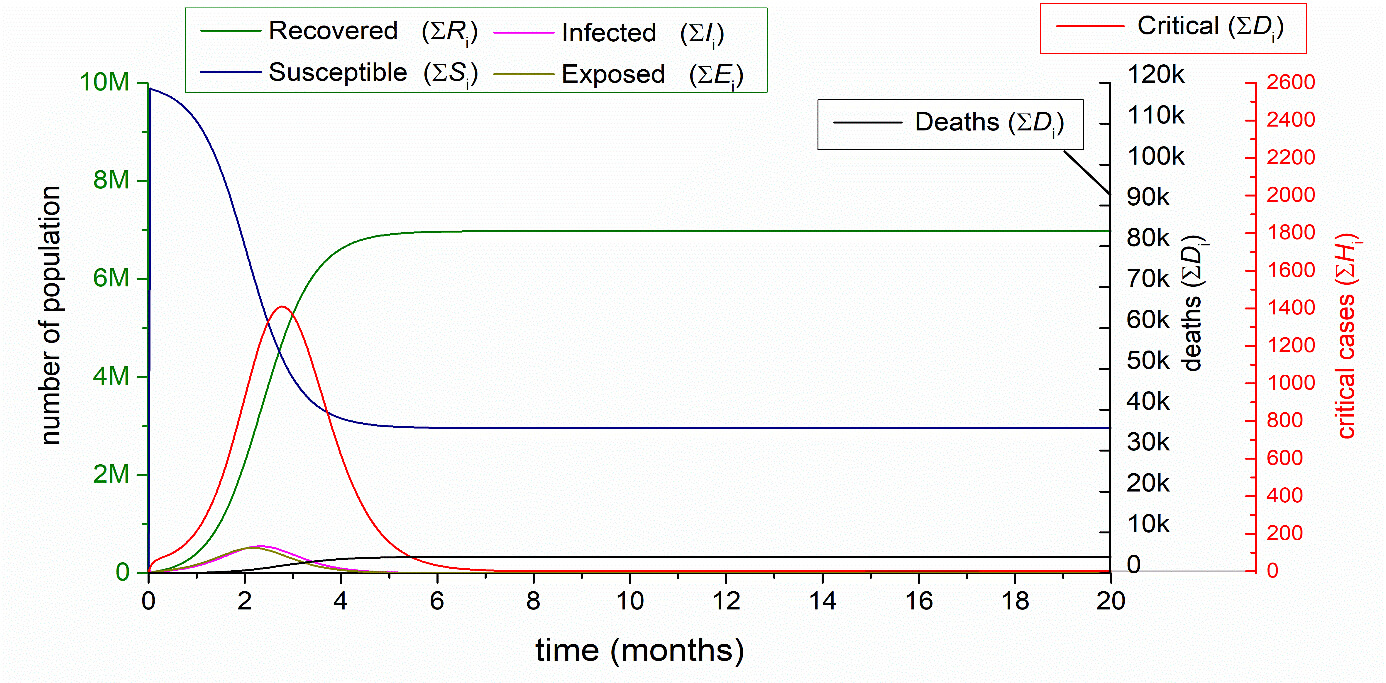
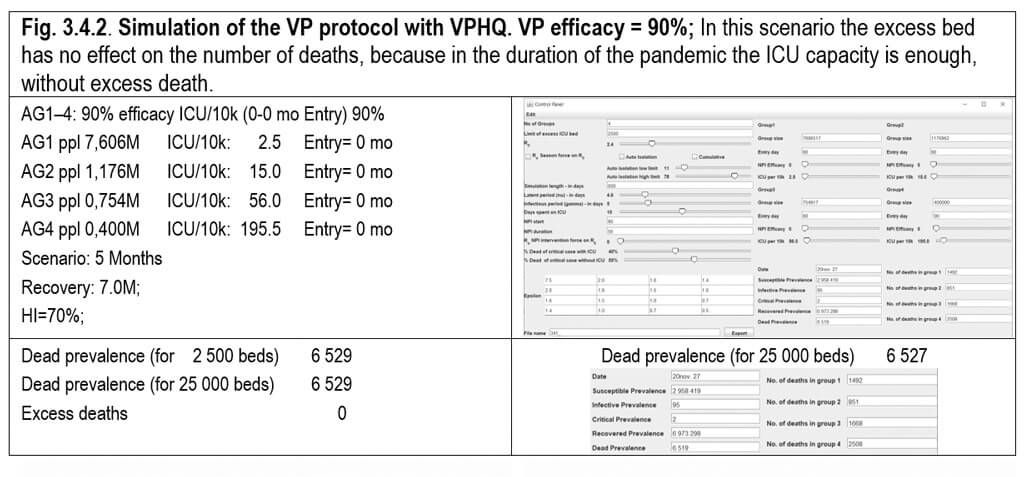

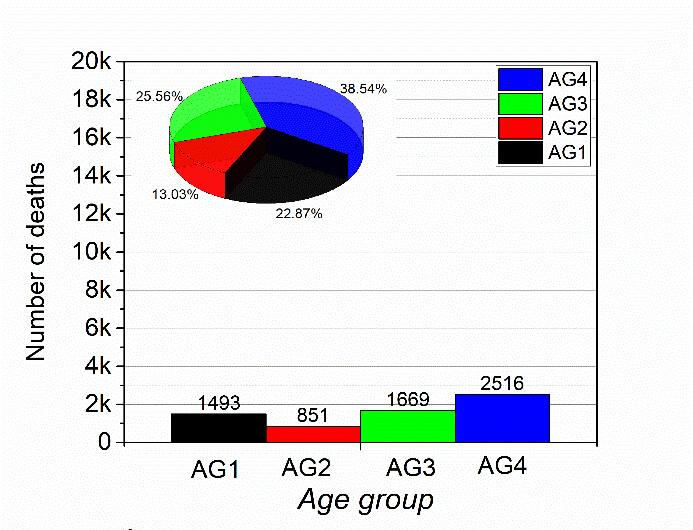

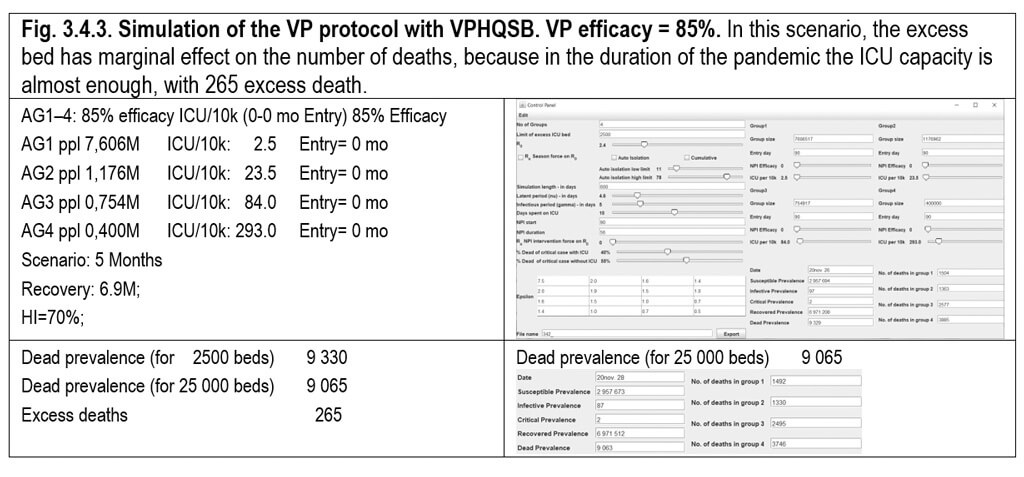



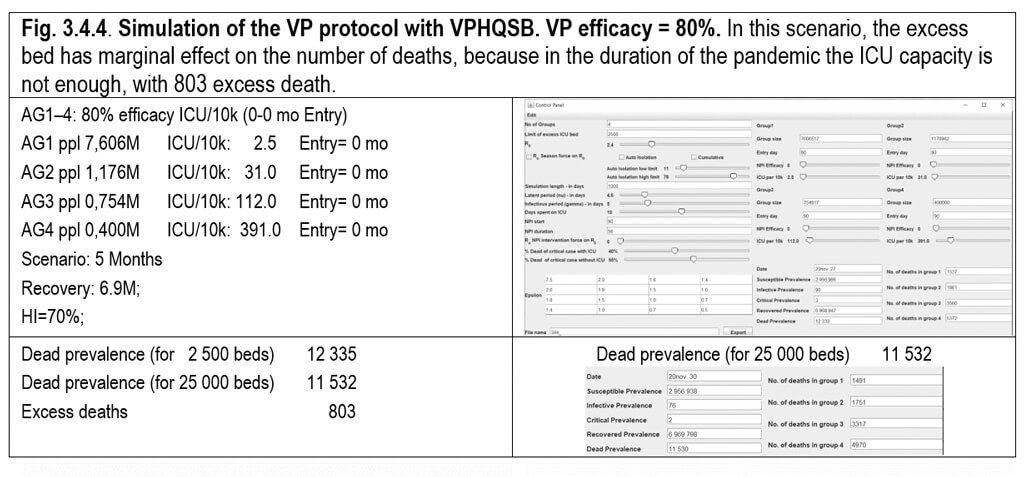



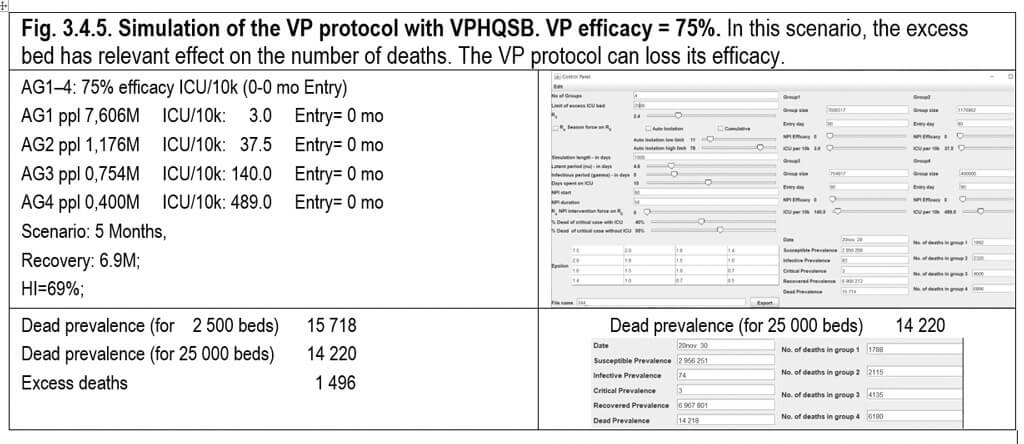



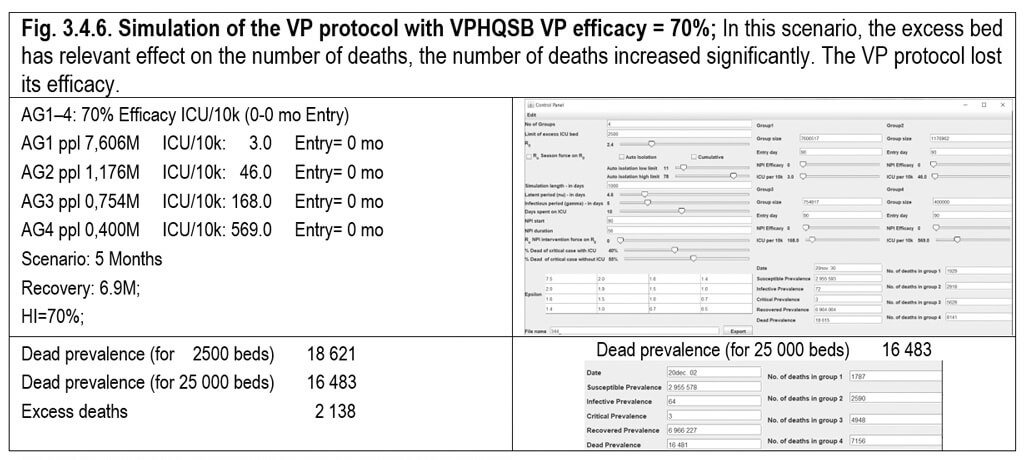

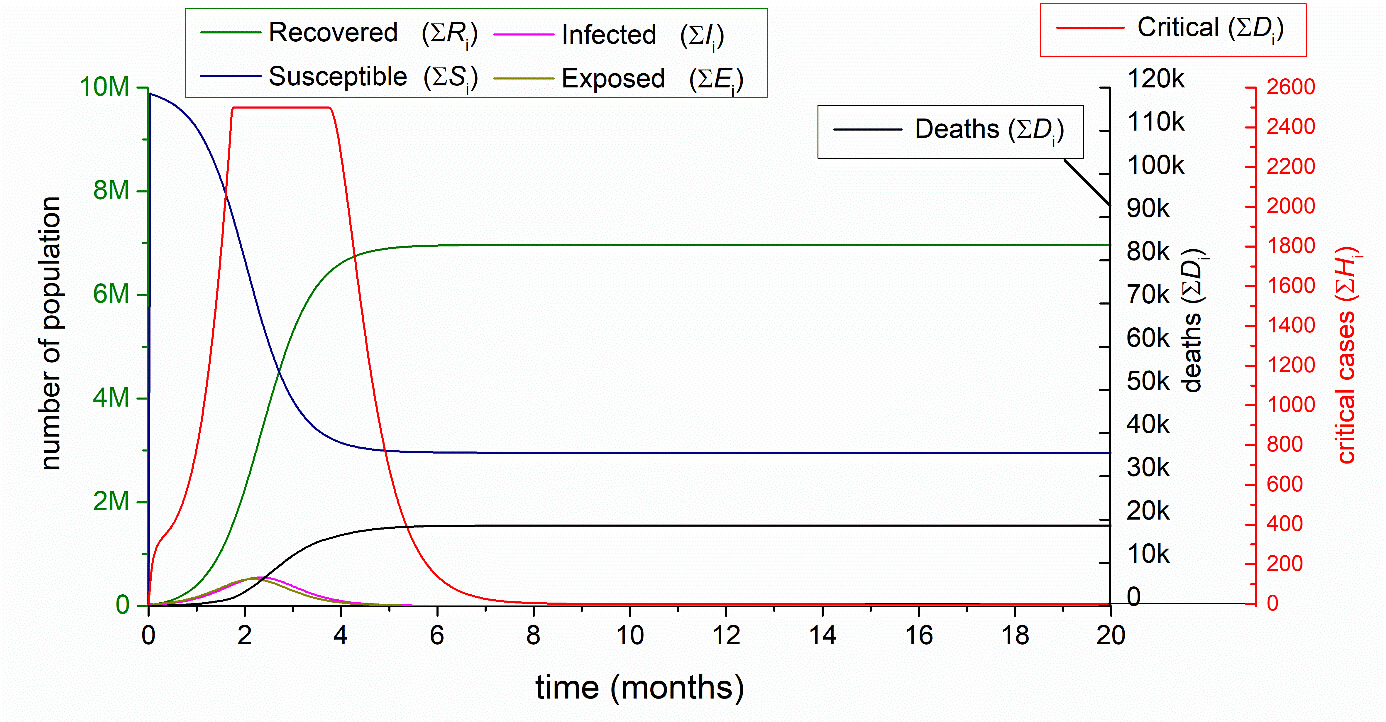
In summary of this section, the VP-ELSE protocol gives a much more flexible and more convenient solution for the management of the pandemic. The method ELSE gives a more manageable freedom of choice, because not the entire population of the related EM AG is regulated under the strict military control. The VP protocol is a very effective method to reduce the number of deaths and besides the appropriate development of the HI. It does not require quarantine system (EM-entry); at the same time, it demands rigid military control - except VPCRH, where only the transport to the isolation place require rigid military control. The protocol is very sensitive to the degree applied. 95%- grade can decrease the number of deaths by 95%, while the 70%-grade results 74% reduction. However, it should be mentioned that even the 85%-efficacy of VP also supposes strict regulation and the significant limitation on the mobility of the VP, which lessen with 80-75-70% efficacy in accordance of the lessening obedience and control of VP.
Table 3.4.1. Summary of the VP protocol with VPD VPCRH/HQSB in comparison with 3.1.3. Natural outbreak.


Fig. 3.4.7. Summary of the VP protocol with VPCRH/VPD, VPHQ and VPHQSB in comparison with 3.1.3. Natural outbreak (NOB).
The very rigid management system of the previous VP protocol, controlling the society by military framework, is not always feasible, since not all the society is able to maintain the necessary severe regulations. The MIX VP protocol offers a more flexible solution for the handling of the crisis. However, we can conclude, that the best solution is the pure VP protocol, (3.4,), in this mixed protocol, a less severe control is applied for the whole AG ppl in 3.5.1. and 3.5.2. for AG1–3, with the use of ELSE for AG4 (entry =quarantine shift is 5 months), while a less severe control is applied for the whole AG ppl in 3.5.3. and 3.5.4. for AG1–2, with the use of ELSE for AG3-4 (entry =quarantine shift is 6-7 months) as demonstrated in the following four examples (Fig. 3.5.1–3.5.4). The scenario too long.
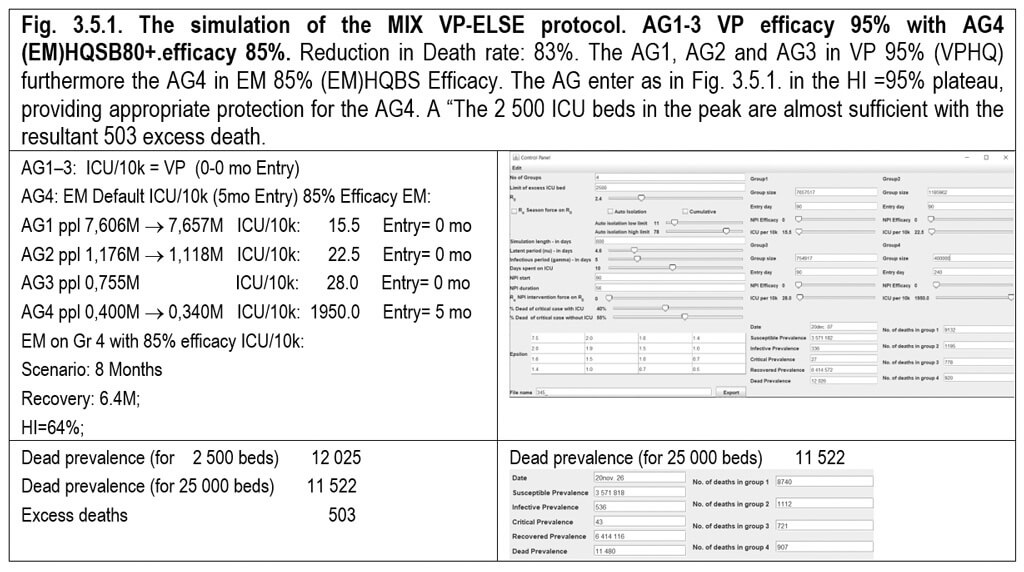


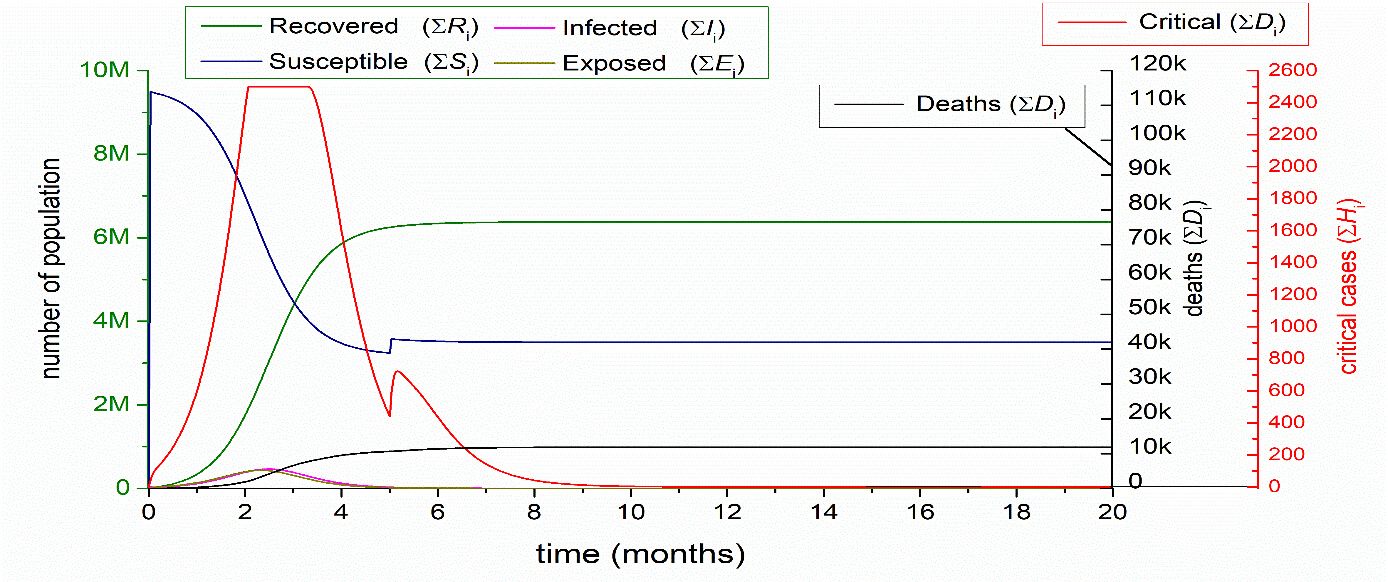

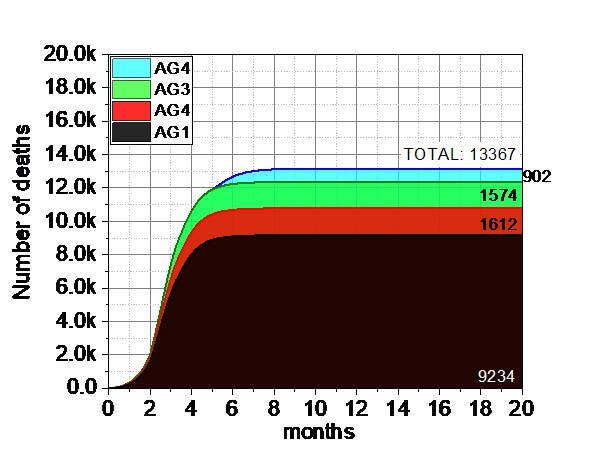





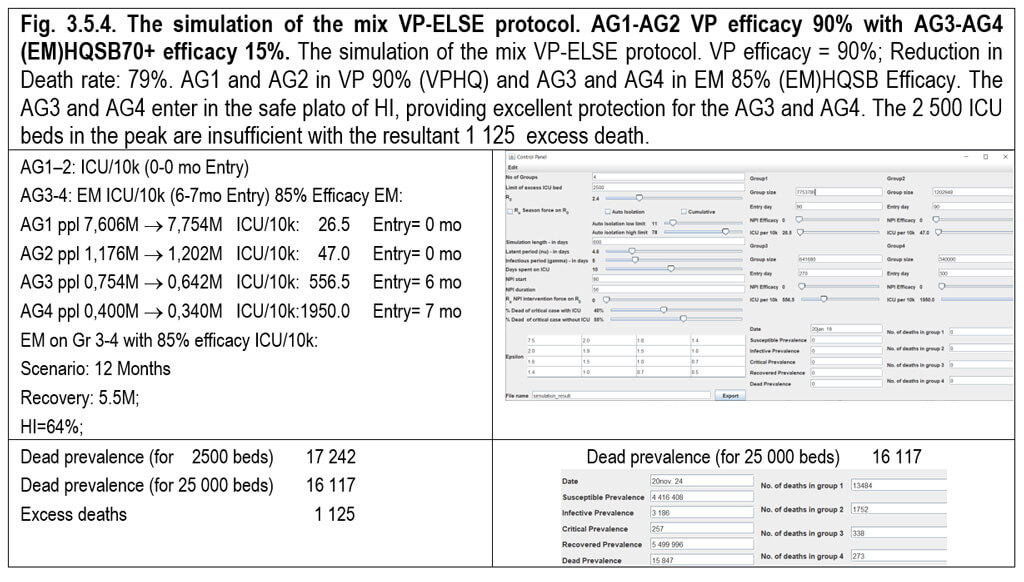
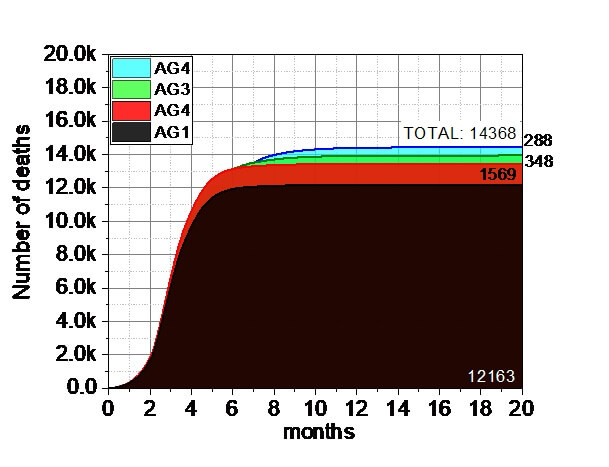
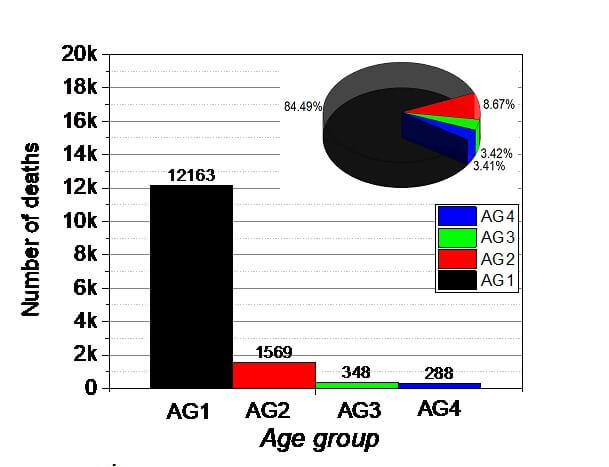

Table 3.5.1. Summary of the MIX VP AG123 95% protocol.
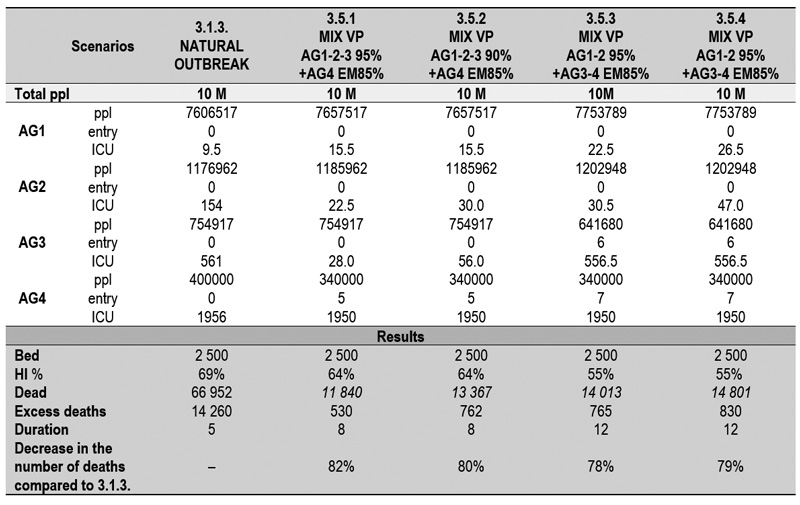
The main conclusion of this chapter is that the longer quarantine does not mean safer protocol. Here, the shorter quarantines with more strict restrictions in 3.5.1 and 3.5.2 may means larger safety.
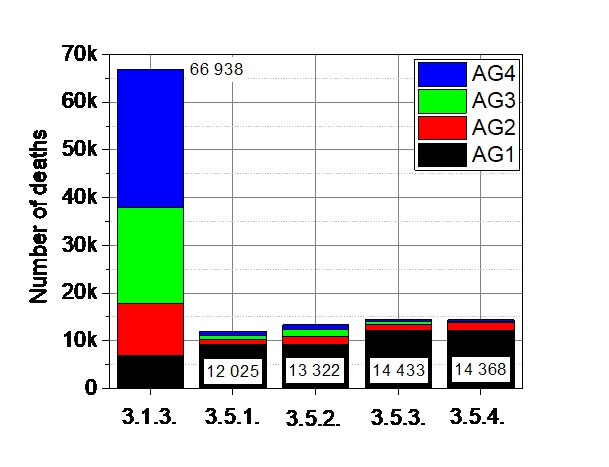
Figure 3.5.5. The summary of the MIX VP protocol represented in sections of 3.5.1–3.5.4.
Here we examined the effect of the entering of the AG4 at the one-third (2.3 mo) as well as at the two-third (3.3 mo) of the HI curve. The NPI has a significant effect to decrease the spreading of the virus. These NPIs includes a wide variety of actions, such as wearing of mask and gloves, keeping the distance, disinfection etc. (Table 2.9.1. NPI not military controlled i.e ELSE and 2.9.2.) To simulate the effect of NPI for the entering of elderly group (AG4), an earlier established mix VP-ELSE protocol was used. In this study, the AG1, AG2 and AG3 are under VPHQ (90% efficacy, entering at 0th mo), while AG4 is under (EM)HQSB80+ protocol (entering at 2.3th mo and 3.3th mo, representing the 1/3 and 2/3 position of the developing HI curves). The number of ICU beds are the standard 2500. The corresponding examples are demonstrated in Fig. 3.6.1–3.6.8. The AG4 enters at the one-third of HI = 69%, providing insufficient protection for them. But the combined effect of the developing HI (at the two third) and the 60% NPI cumulative effect can be as good result, (3.6.8.) than the VPHQBS 85% efficacy (3.4.3.) with ten thousand death.

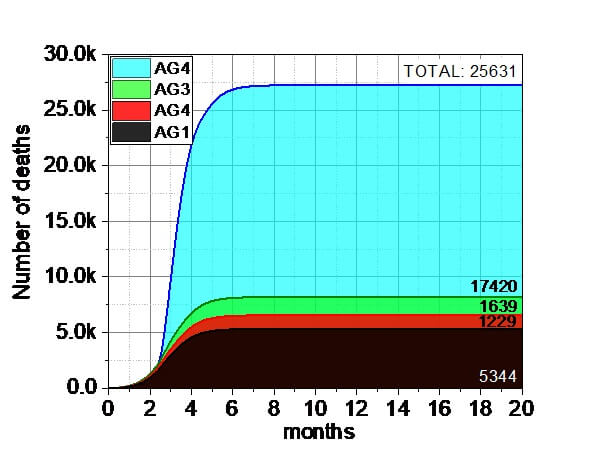
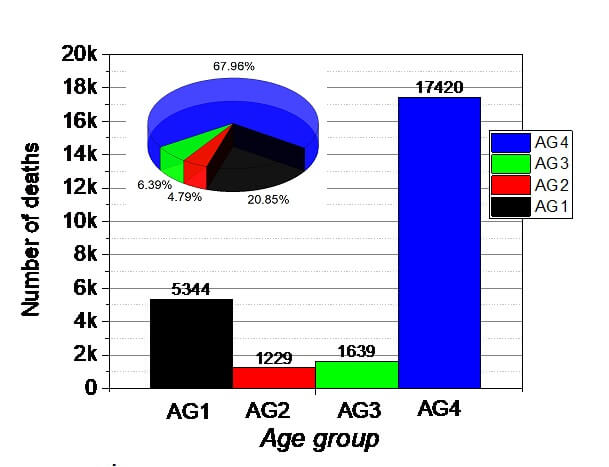
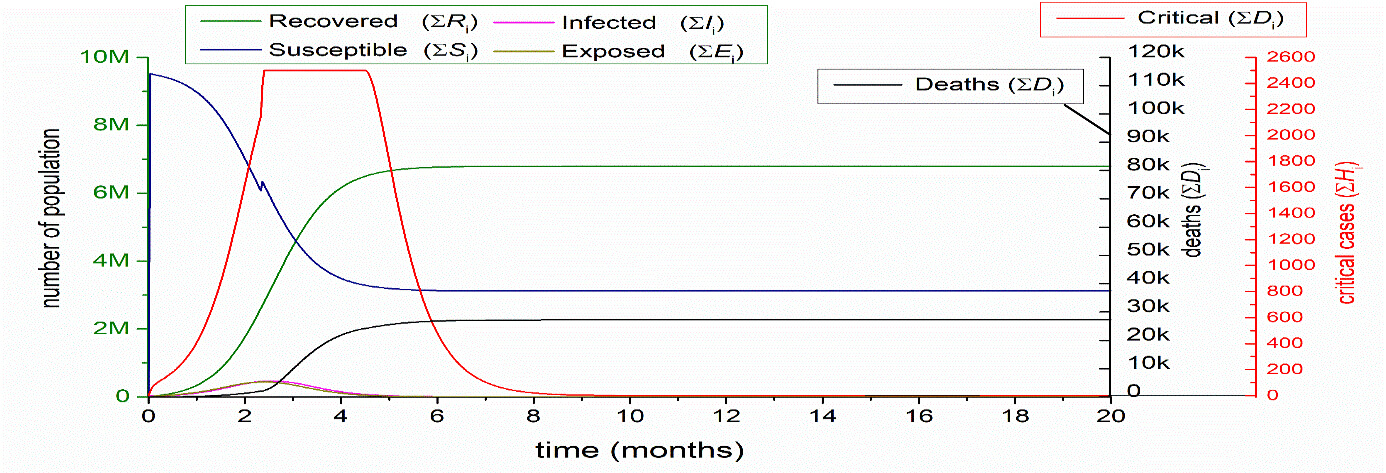
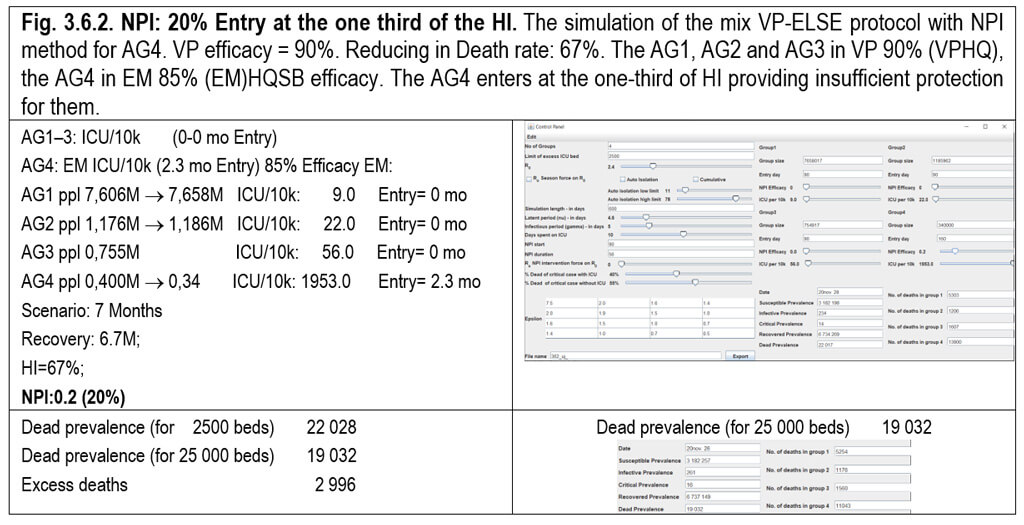


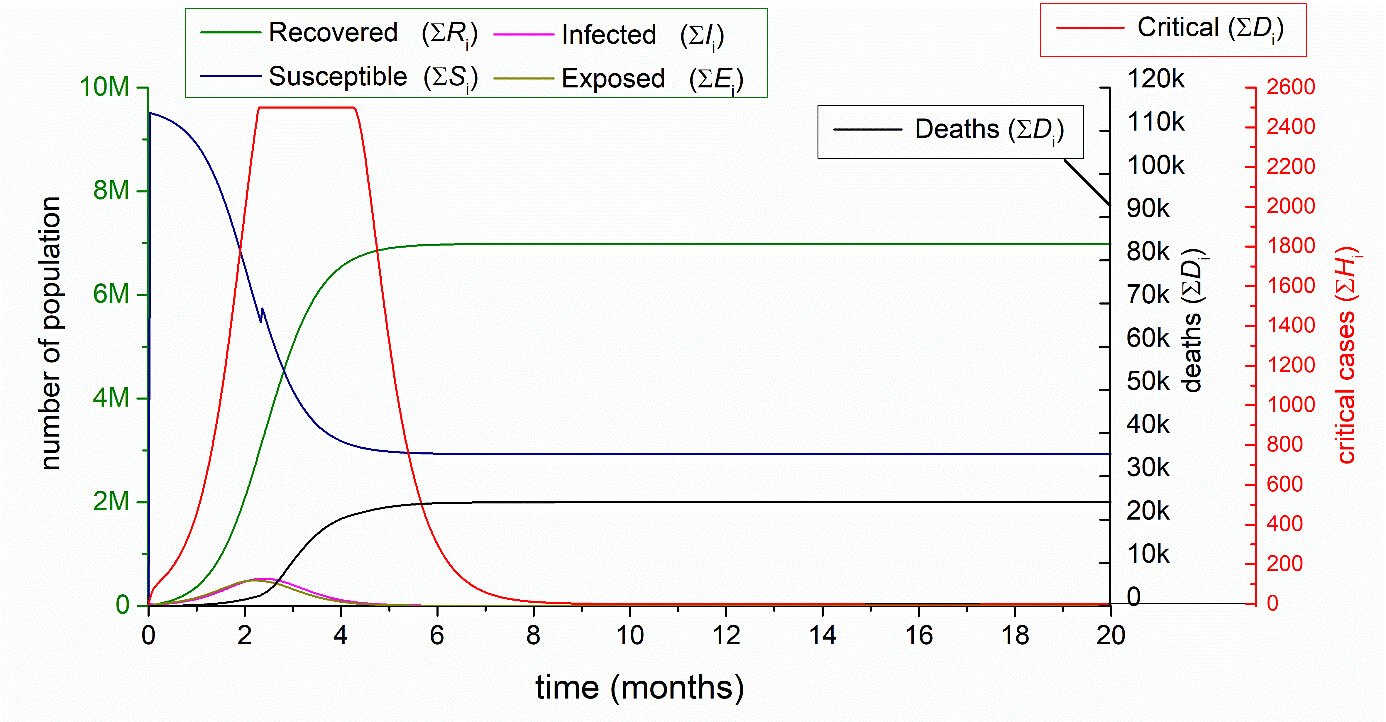

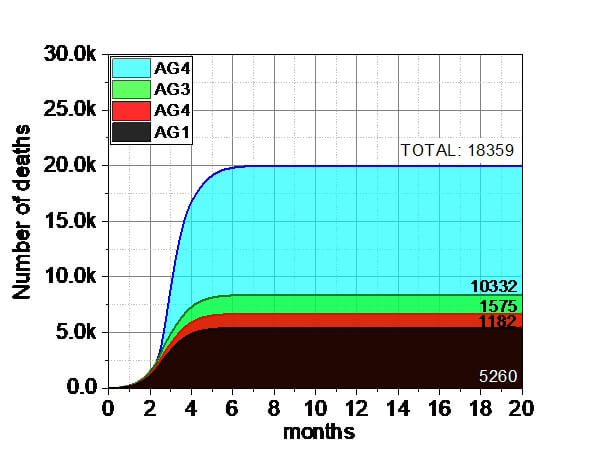
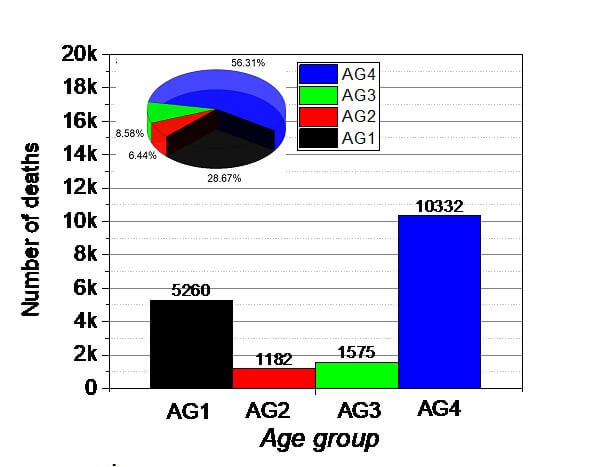

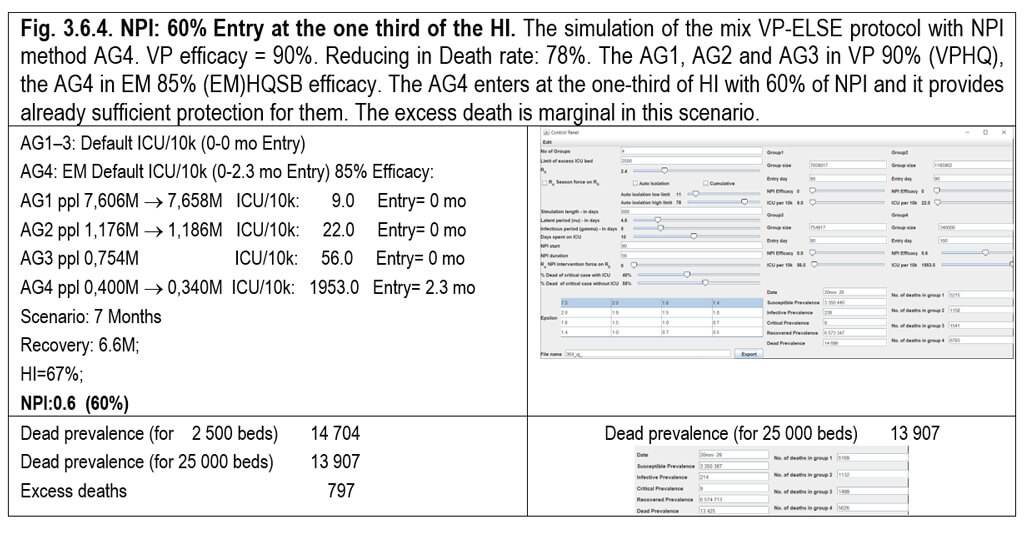
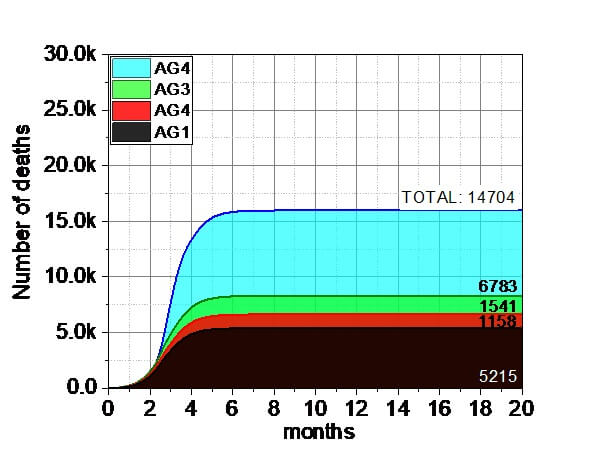


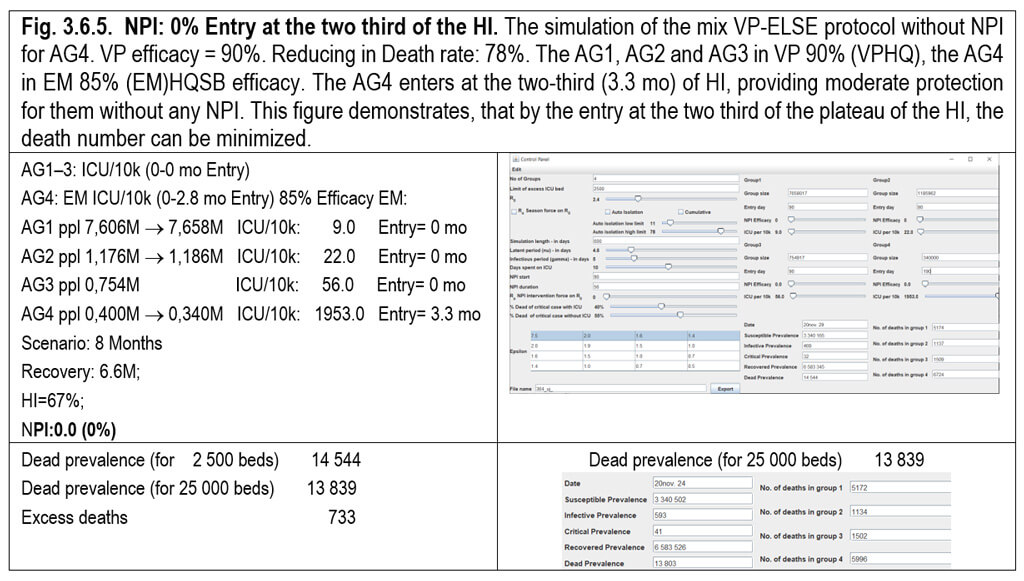
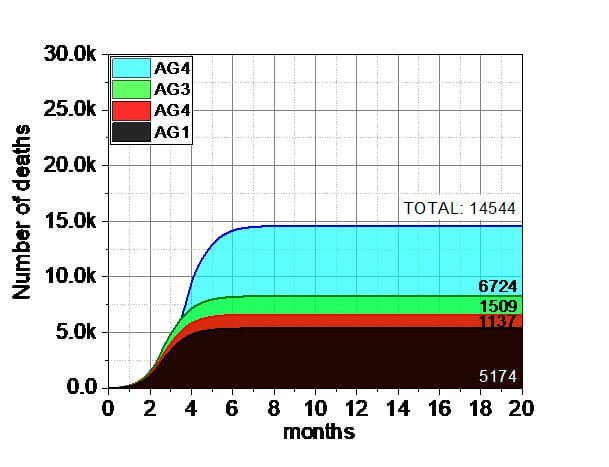

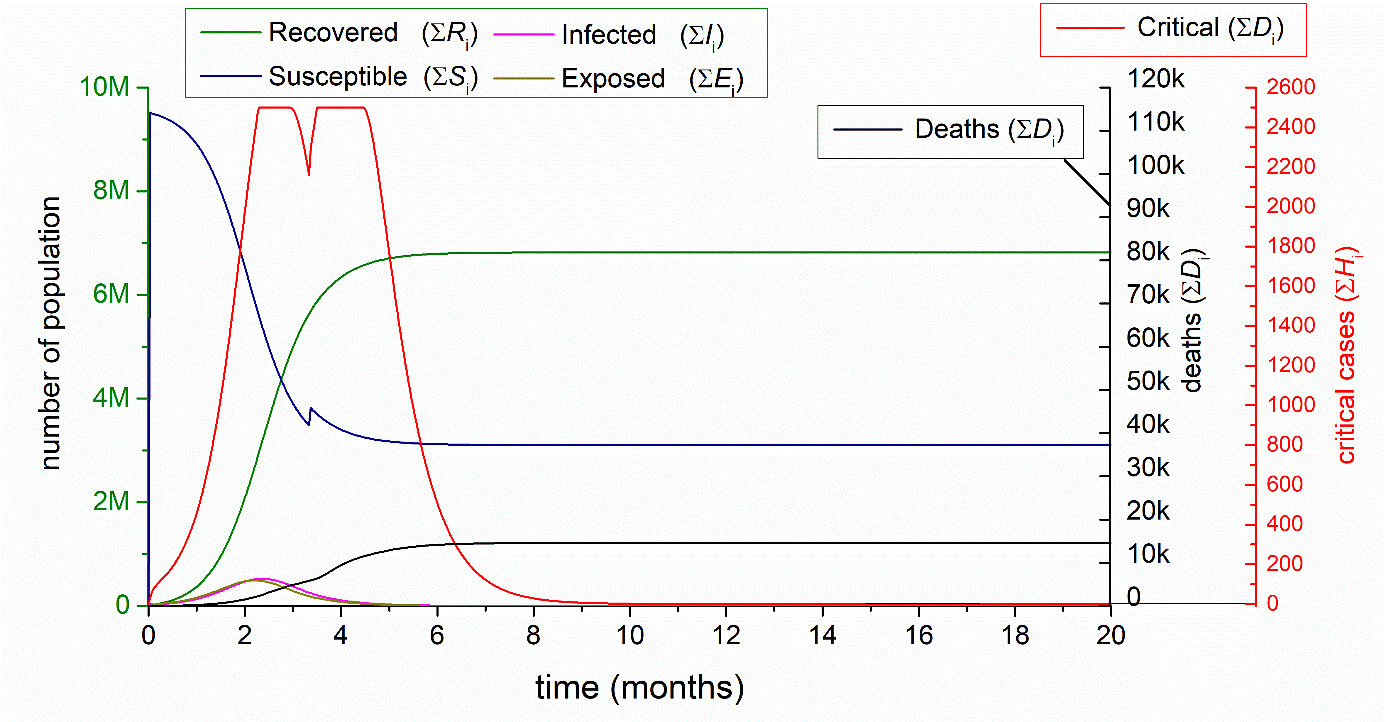
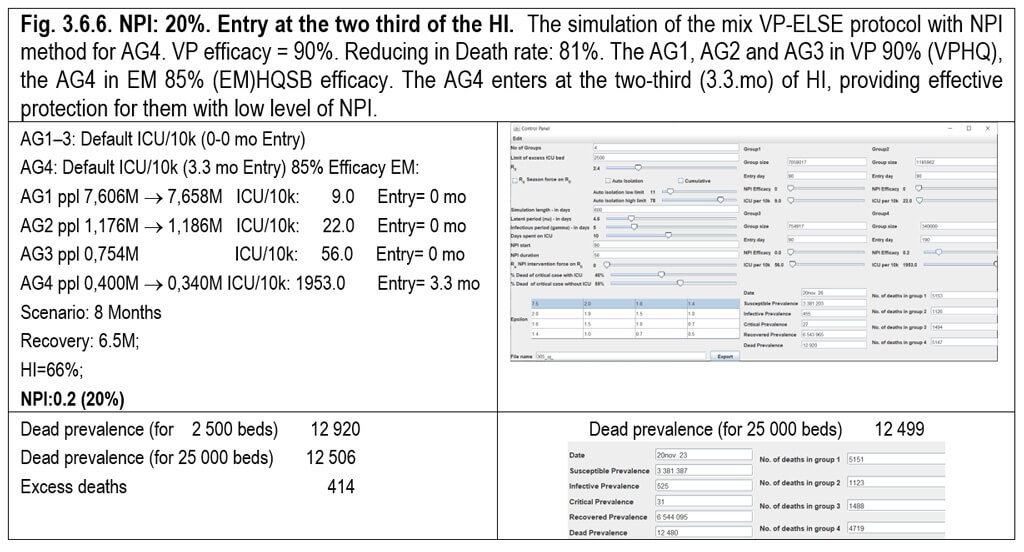
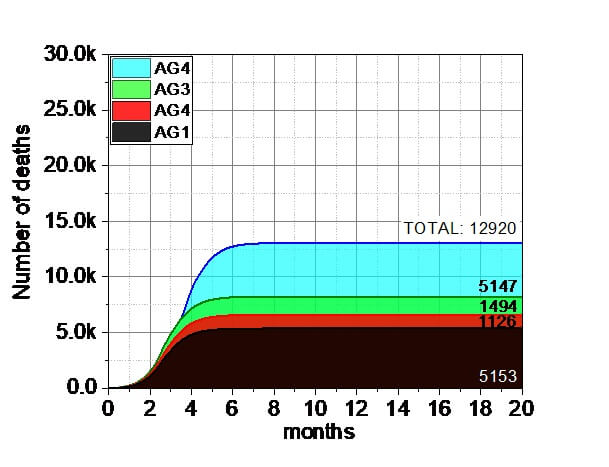

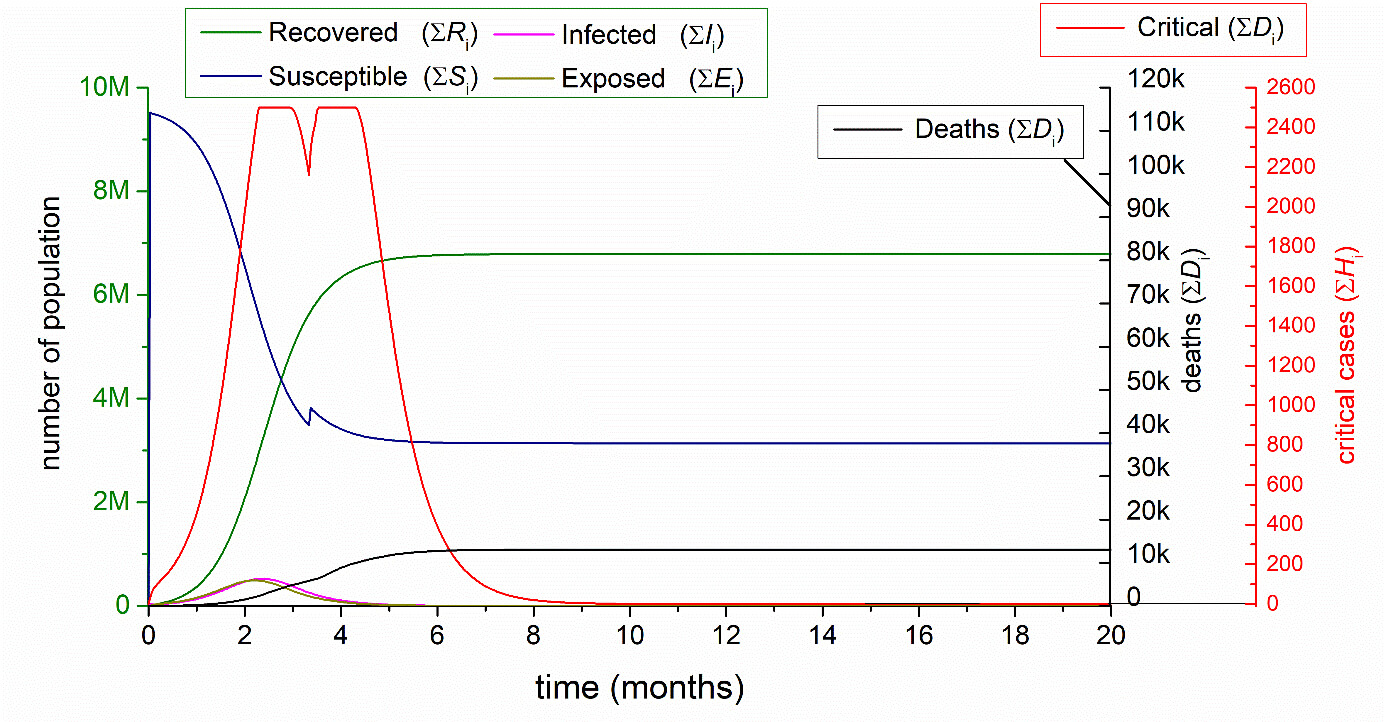
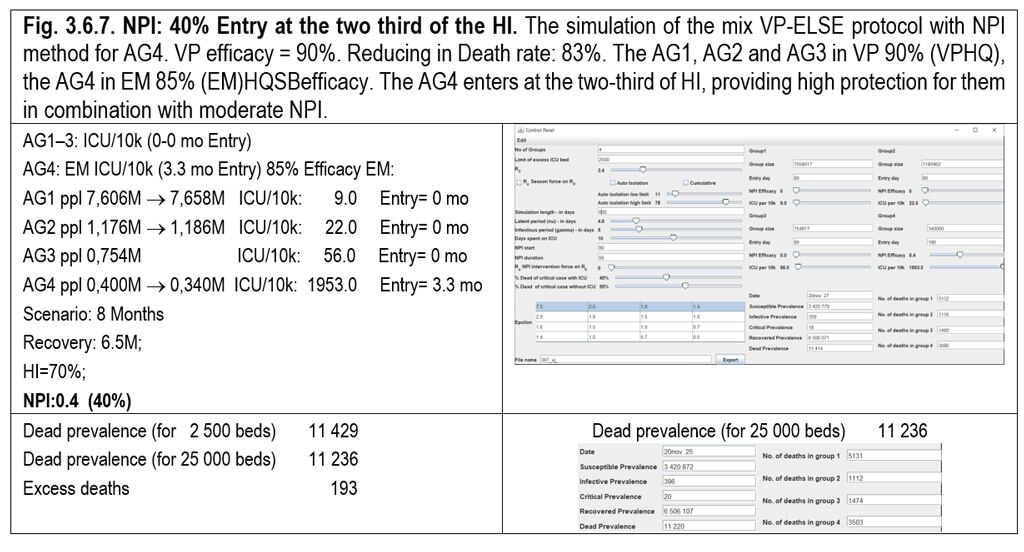
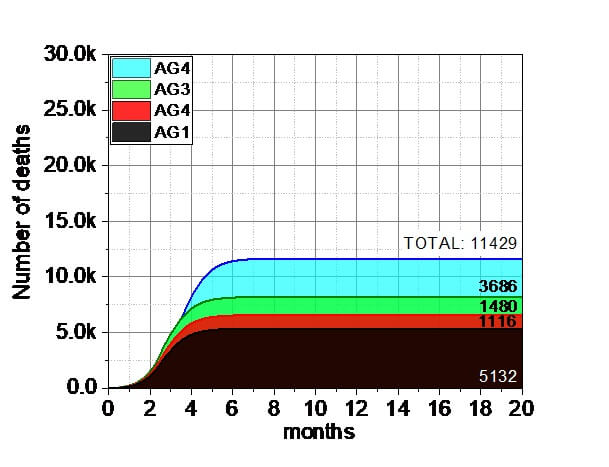


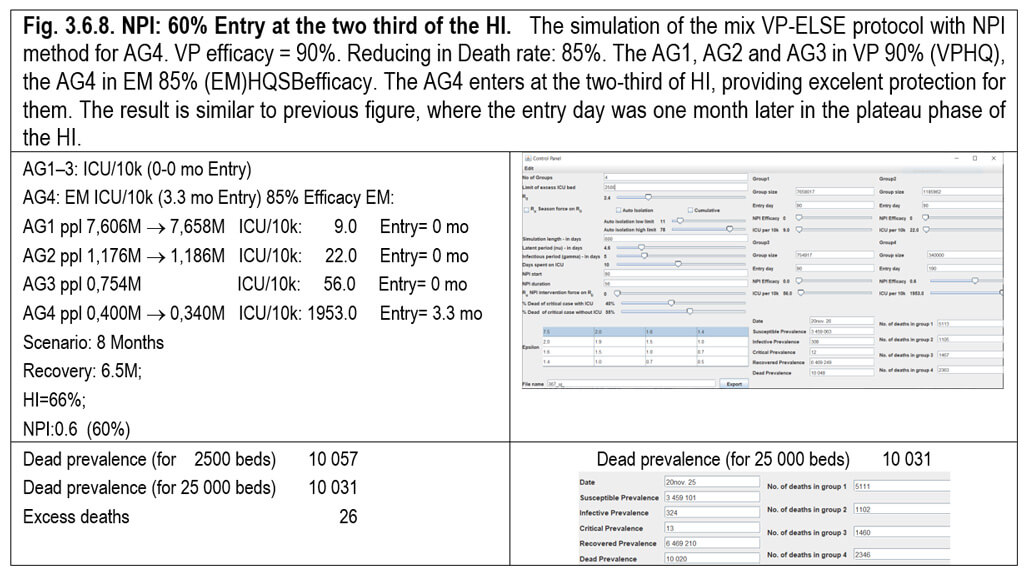
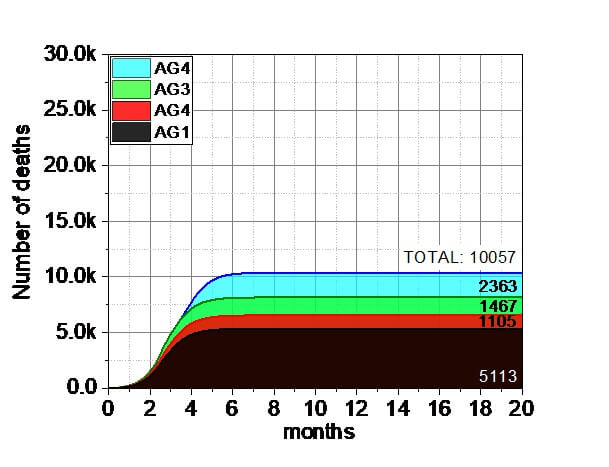


In summary, it is obvious that the increasing NPI values of AG4 result decreasing number of deaths, because it inhibits the spreading of the virus from the infectious people to the susceptible. The effect of the NPI is more dramatic for the earlier entry of the AG4 at 2,3 mo, because the HI reached only its one-third value, resulting more significant infectious in the AG4. However, the later entry of the AG4 at 3,3 mo exhibited reduction in the number of deaths, representing the invincible role of the HI.
Table 3.6.1. Comparison of the number of deaths respect to the NPI value of the AG4 (3.6.1–3.6.8).
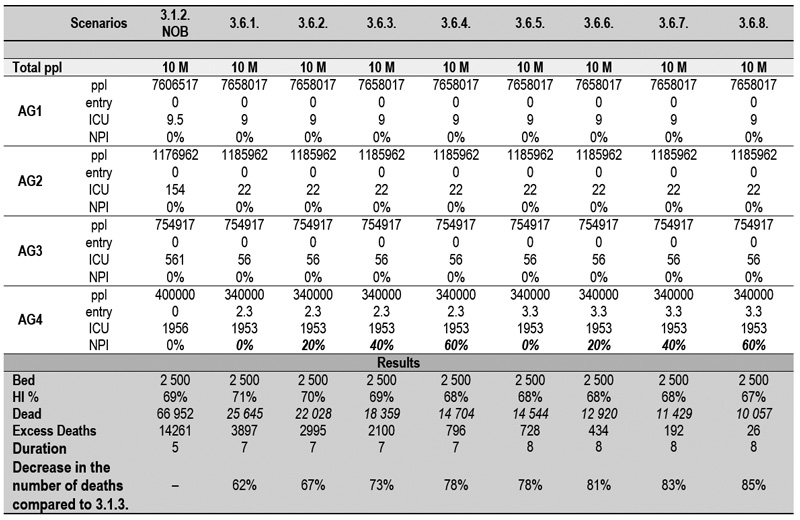

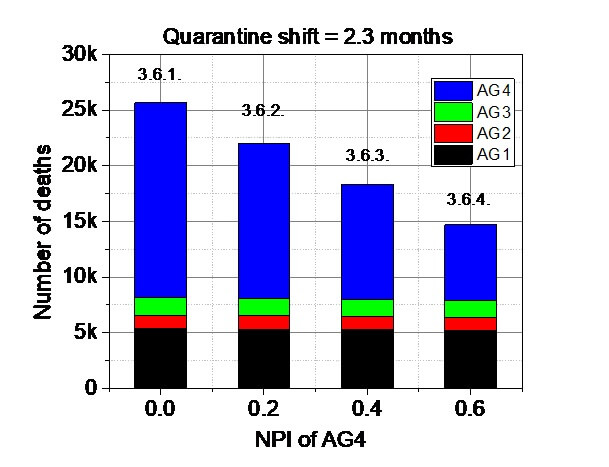
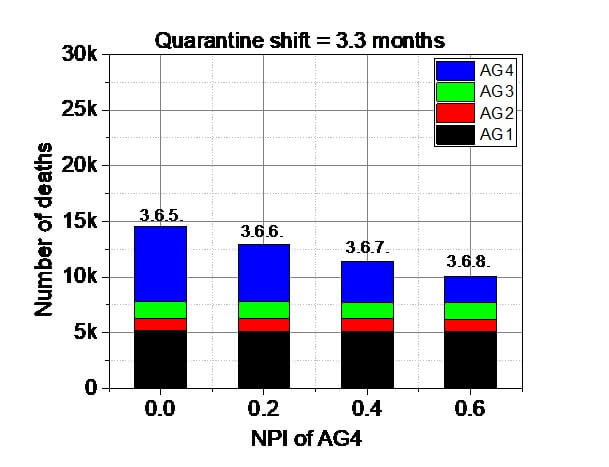
Fig. 3.6.9. Comparison of the number of deaths respect to the NPI value of the AG4 (3.6.1–3.6.8).
Here we examined the effect of the entering of the AG3 and AG4 at the third (2,3 mo), at the half (2,8 mo) , at the two-third (3,3 mo) and at the plateau(4,3 mo and 5,3 mo) of the HI curve. The AG1-2 in VP isolation with 90% efficacy while the AG3-4 in 60% NPI for the whole ppl after the different quarantine shift =entry.
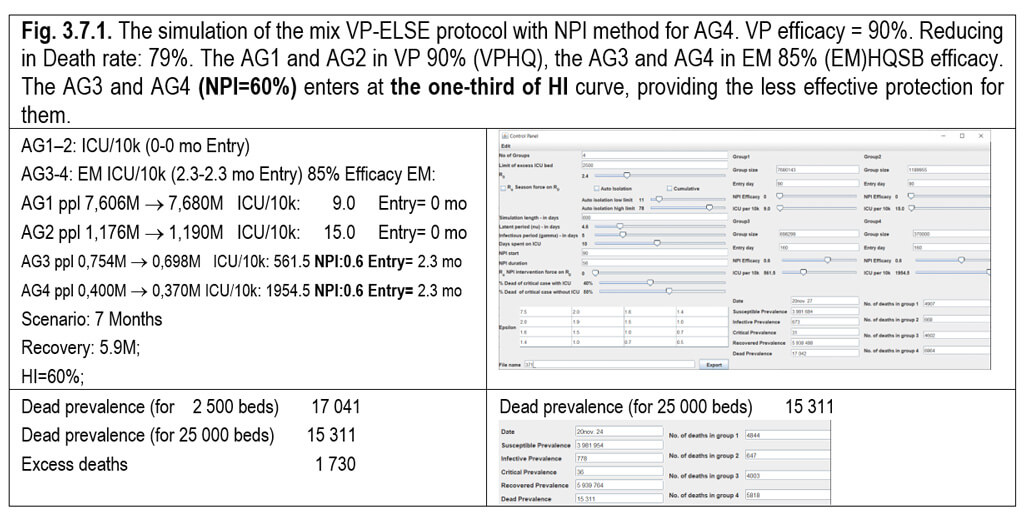
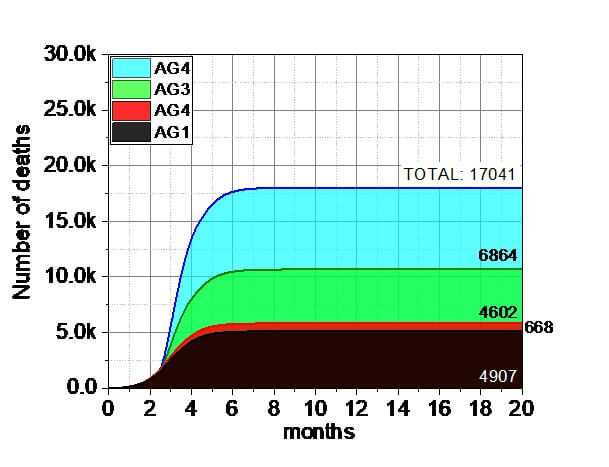

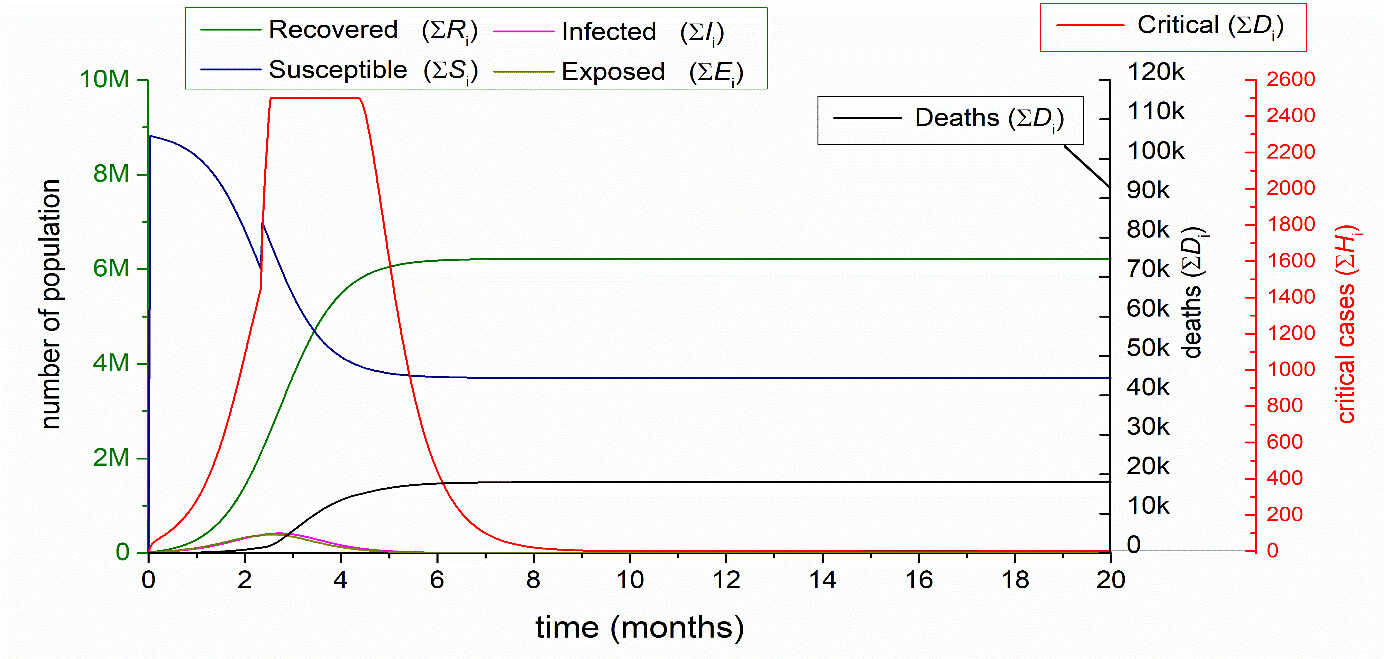

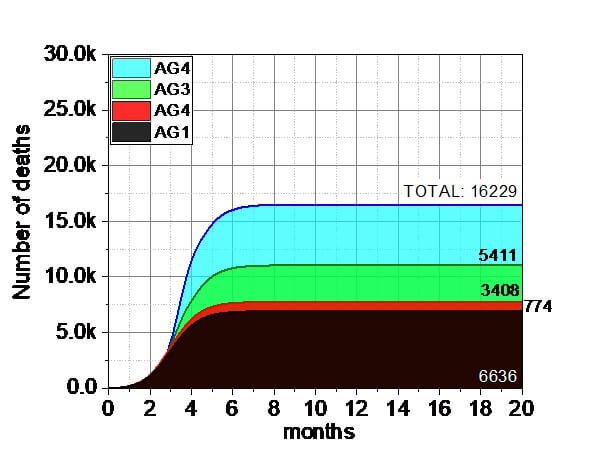
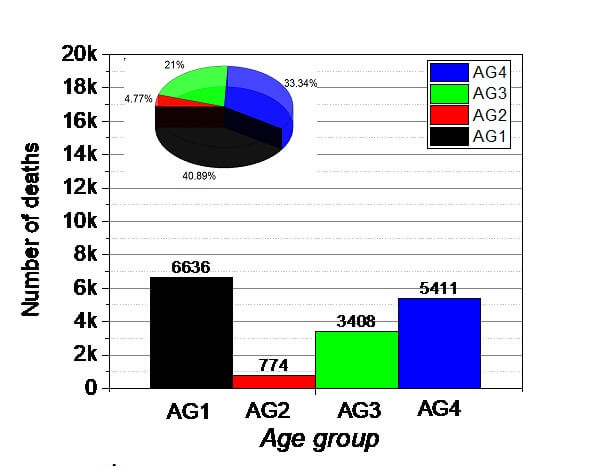

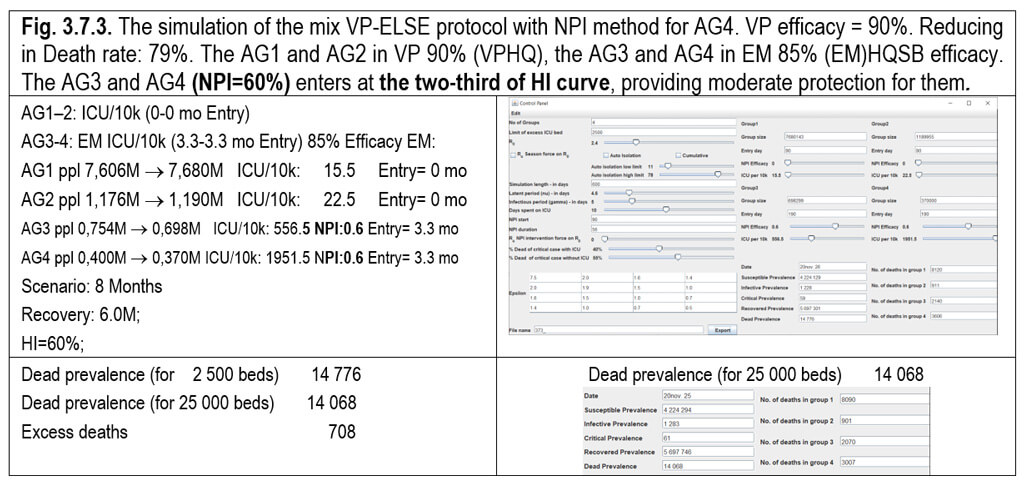

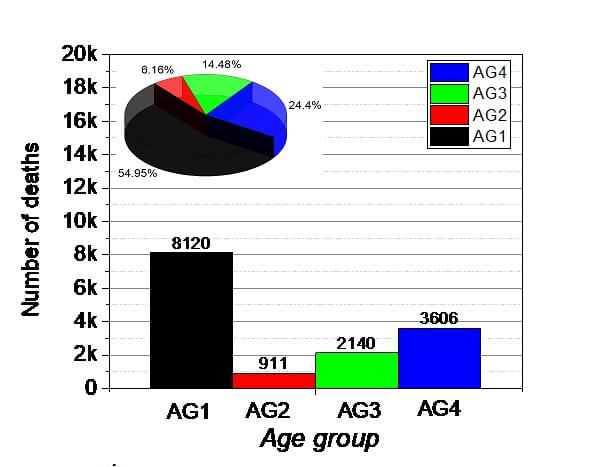



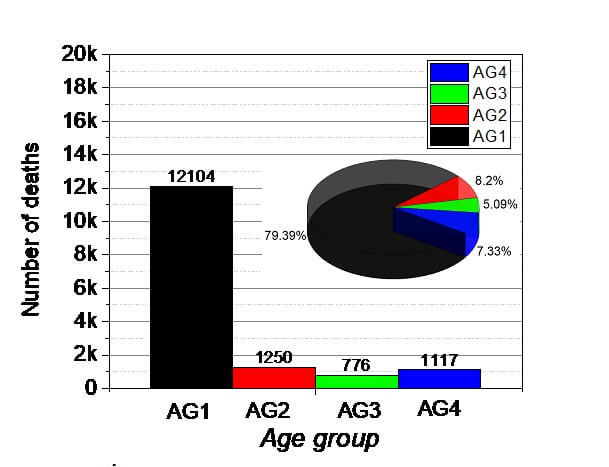

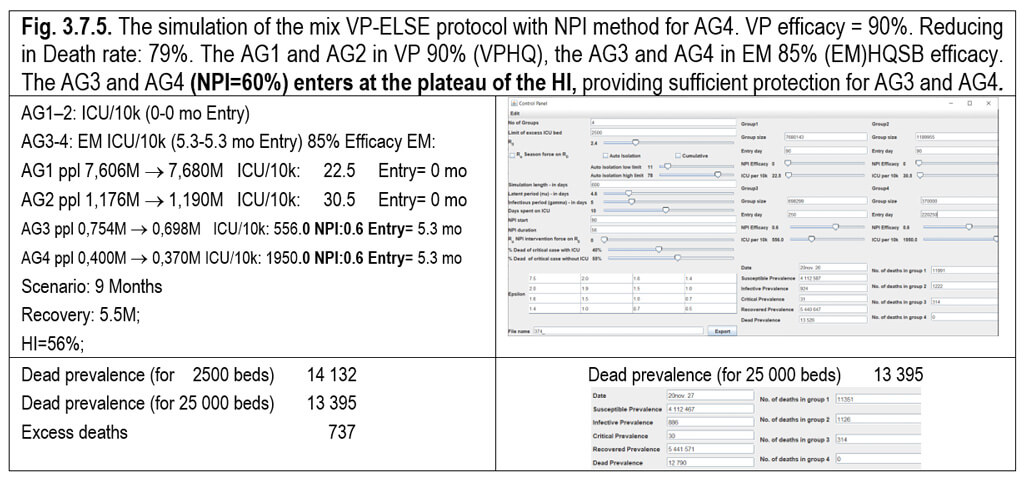



This section demonstrates the effect of the NPI for AG4 in Table 3.7.1 and Fig.3.7.5.
Table 3.7.1. Comparison of NPIs
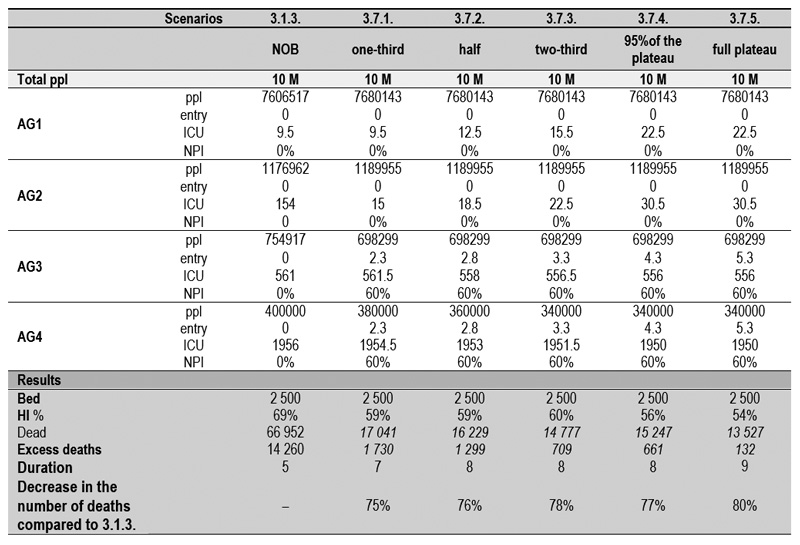

Fig. 3.7.6. Comparison of the NPIs of the section of 3.7. It demonstrates that it is not trivial to find the optimal parametrization of the quarantine period vs VP protocol. Further, it depends on the country, the populations and its distribution.
Summary: This book tries to explore all essential possibiities to eradicate the SARS-CoV-2, and to stop the global socioeconomic disaster. It is apparent that only VP isolation can offer the most efficient and in addition most cost-effective solution. (3.4.1.-6.) Among the members of the society only a fragment (72-600 / 10k, that is 0.7-6%) should be isolated or subjected to restriction, while the rest of the society (94-99.3%) can immediately live a normal life. Any of the appropriate and/or affordable VP protocol versions (3.4) can be implemented anywhere in the world where GPs and immunized i.e. vaccinated soldiers and/or staff are available. For the time being abundant number of protected candidate, staff are obtainable through natural infection and/or by vaccination.
Other NPIs can also significantly influence the development of the pandemic toward favorable directions and decrease the number of deaths or shorten the period. However, any combination of NPI and quarantine shift (scheduled entry) of AG3-4 will never reach the efficiency of ELSE VP protocol (3.4.).
Except the MIX VP protocol (3.6.6.-7.-8.), where the AG1-3 are in VP isolation and the whole AG4 (400/10k) is in (EM)HQBS80+ in a scheduled early entry (3.3 mo) with the subsequent 60% NPI. For any reason if it is not possible to isolate the AG4 VP (78/10k, with excess II = 156/10k or excess III = 234, more than half of the total ppl of th AG4), than the most effective way to force them in VPHQBS80+. From this possibility either the developed or the developing countries can decide – according to the current epidemiological and/or socioeconomic situations - the choice to manage the actual situation. One of the 3.6. for all AG or for example AG1-3 VPCRH and for the AG4 a quarantine shift of 3.3 mo entry and 60% traditional NPI. All of these protocol, comparing to VP protocol (3.4.) needs more continuos military discipline and cots. (except VPCRH).
Irrespectively, from the evaluation of the pandemic dynamics of SARS-CoV-2, the measurement of the real data is undoubtedly required to understand and management of the current processes. As a good news, the unexpectedly rapid development of the vaccines offer a breakthrough. However, their effective spread will takes months and the developing world a year. This is a long time with still millions of death and turmoil. Based on the accumulated international experience, governments are trying to address the dramatically rapid pandemic flow with many different and virus dictated restrictions of suppression and/or mitigation, affecting a huge section of society. Nevertheless, this direction will have several predictable negative consequences. In this section, we modelled several pandemic scenarios in a logical system in order to select the optimal intervention to protect the endangered population (VP), meanwhile the economic and social costs are minimized.
Also, crucial aspect, that any of the strategy selected can be adapted anywhere in the world at any stage of a pandemic, based on the current epidemiological and demographic status and the logistics, declaration of enforceability parameters.
The first element of our investigation is to reduce the burden of the healthcare system and makes it allow to care the non-virus-related urgent cases.
The second and more important element to prove that the generation of the appropriate level of the herd immunity, with boosted by the meanwhile developed safe vaccine could be the only way to eradicate the SARS-CoV-2.

Fig. 3.8.1. Short summary of the numerical models of the pandemic, discussed in the paper. The chapter numbers are indicated on the vertical axes the horizontal axes indicates the No of death relates to 10 million population. Therefore for example, the max. No of death 72 411 is equal to 72,5/10k (Chapter 3.1.1.), and the the min. No of death 4 020 is equal to 4/10k (Chapter 3.4.1.) Nat Out = Natural Outbreak; ELSE = Elderly Life Saving Emergency; VP = Vulnerable population; NPI = Non-Pharmaceutical intervention.
Important considerations:
- From epidemiological viewpoint, the most important conclusion is that the combination of interventions which creates, as high as possible HI level as soon as possible, results the most acceptable and optimal outcome, because the HI is the most important protective factor in the long term.
- The HI can be considered in a population level (HI=1-1/R0) as a protective “naturally developed NPI” mode, because the person, who underwent the disease infection and recovered is protected completely. These protected individuals are playing similar like the 100% NPI efficacy (= the individuals are not able to infect anybody and and not able to be infected by infector). They represent no infection potential for the rest susceptible individuals, in a person-to-person relationship. The HI and the NPI (2.9.1.) have together and cumulative protective effect. In a population, for example, if HI = 30% is at a protective level combined with any other NPI is 30%, the cumulative total effect could be 60%.
- If there is no opportunity to raise the HI curve to a certain level, - and the plateau flattens below the required HI level, or even below the level of the death curse – the number of deaths become significant.
- For this reason, maximum efficacy by HI could be achieved by starting at least the AG1 and AG2 groups, representing together the largest portion of the population (88%) with the lowest VP (17%) at zero day (day 90). (section 3.2)
- If the starting ppl in the AGs different, than the default, their ppl number should be at least 70% of the total population of the country or area, if R0 is around 2,4.
- The rapid development of the pandemic situation causes a significant mortality rate from the AG1-2 (3.1.6). If the VPD and/or VPCRH can not be applied in the AG1-2, then we need to consider the ethical maximum during the development.
- When, without isolation of VP from the AG1-2 (total ppl) vs AG3-4
- Only scheduled entry of (EM)HQSB of the AG3 and AG4 is investigated, it means that 10k of the VP in AG1 and AG2 [from the 7k + 18k = 25k] will be sacrificed, in order to generate a rapid high plateau of the HI. (3.1.5.)
- The VP /42k+78k/=122k of the AG3 and AG4 will be survived during the pandemic, by the appropriate entry after the development of the plateau of the HI, providing safe protection.
- However, this 10k sacrifice of the AG1 and AG2 commitment can be avoided, by significant postponement of the scenario, but it could bet unsustainable and unsanctionable maybe for a year (3.3.)
According to the presented results, especially the number of deaths, we could conclude the following points. The worst scenario corresponding to the Natural Outbreak (3.1.3. ICU beds: 2 500, R0 = 2.4, IFR = 0,9%, Death: 66,9/10k), used as the reference point for all the models discussed.
Table 3.8.1. A systematic concise comparison of the various protocols discussed in the result section. The colors refer to the number of deaths predicted. (From /high red/ to /light red/ to /yellow/ to /green/
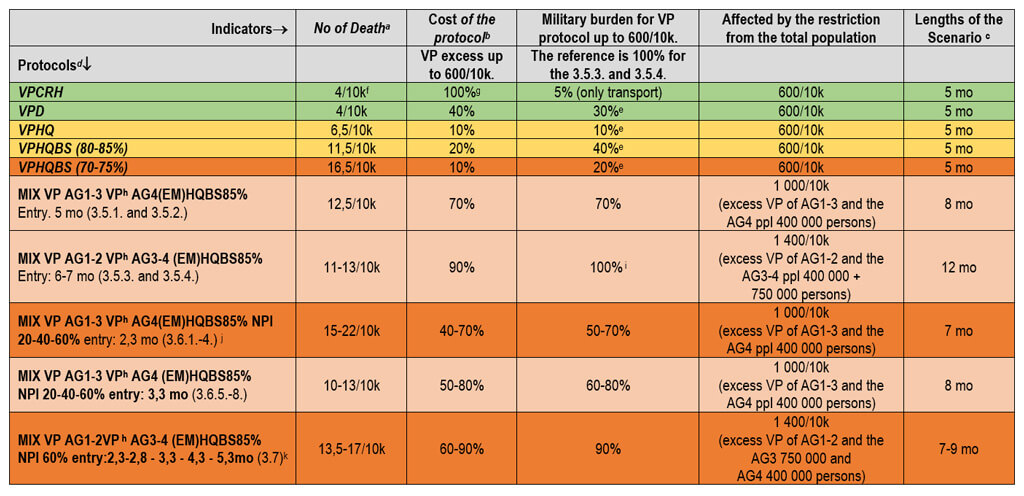
a Most critical indicator of the pandemic;
b for prices see 2.7.1.
c Duration of the pandemic (i.e. epidemic, if performed in certain area) model.;
d The 3.2. and 3.3. are not included, because all of the indicators are fare more the worse, compering to the others;
eThe less military burden are in the VP protocol;
f4/10k number of deaths represent the results for the most effective isolation;
gThe most expensive scenario, but it is still less than the health expenses ;
h The VP efficacy 90 and 95%;
i The highest military burden as reference 100%;
j Due to the non-controlled scenario (keeping social distance and avoiding contact behavior, reduced vaccine compliance etc) that has developed, it will be longer time, but the relative ratios would be similar regardless of the time of the scenarios;
k After the 2,3, 3,3, 4,3 and 5,3 mo with 60% NPI the scenario lasts altogether 7-9 mo. In the case of 4,3 and 5,3 mo entry in the plateau of HI the NPI is almost unnecessary.
ELSE EM 100% efficacy (3.2) is a theoretical approach that do not exist in the real life and were analyzed as a comparable reference.
ELSE EM Protocol with 85% efficacy (3.3) protocol can use if there are no way to identified and/or isolate the VP.
- It decreases the number of deaths, meanwhile the HI can also develop to the demanded value (>55%; R0 = 2.4 = 58%). The number of deaths greatly begin to reduce, as the entries reach the plateau of the HI. (3.2.1, 3.2.2. and 3.2.3 vs 3.2.4 and 3.2.5). Moreover, the duration of the pandemic situation become gradually longer with the later entries.
- However, the efforts and cost are higher than the application even the VP protocol of 3.4.6. with 70% efficacy, which offering significantly less death with several months shorter scenario and forcing significantly less individuals subject to restrictions.
The VP -ELSE Protocol (3.4) exhibited the lowest death count and the number of people to be controlled is the lowest of all versions.
- It is a very effective method to reduce the number of deaths, offering a much more flexible and more convenient solution for the management of the pandemic.
- It provides an appropriate development of the HI.
- It does not require the EM-entry quarantine shift system (EM-entry) for the whole ppl of the related AG.
- It gives a more manageable freedom of choice, because significantly less individuals should be controlled.
- The protocol is very sensitive to the degree applied. 95%-efficay decrease the number of deaths by 95%, while the 70%- efficay results 74% reduction.
- The necessary rigid military control required in:
- o VPCRH – only a limited time for the transport of them to the isolation place.
- o VPD, VPHQ and VPHQBS with 85-80% efficacy
- The rigid regulation and limitation on the mobility of the VP lessen with 75-70% efficacy in accordance of the lessening obedience and control of VP.
- VPCRH: (3.4.1.) Distant home isolation. The most reliable and effective (95–98%) version, with the highest cost of all is the VPCRH, led to 4/10k death cases, with IFR= 0.05% respectively. The VPCHR require a one-time strict control, to transport to the Cruisers, Resorts and Hotels. Afterword the protected staff can fulfill the maintenance tasks.
- VPD AND VPHQ: (3.4.2) Isolation tied to home. The second reliable and effective (90–95%) version, with moderate cost are the VPD and VPHQ, resulting 6,5/10k death cases with IFR= 0.08% respectively. It supposes severe and rigid militaristic control, which is hardly maintainable in the developing part of the world.
- VPHQSB: (3.4.3.-6.) Isolation tied to home. The third reliable and effective VPHQSB version with the lowest cost can implement the easiest way, almost one day to another. Inspection and disinfection of designated buses and shops that operate not in the time zone, but preferably throughout the day, can be easily solved and more effective. Logistics is the simplest. This is furthermost recommended for developing countries.
i. If the 85–80% efficacy could be maintained the death rate would be 13/10k. IFR= 0.16% respectively. (3.4.3. and 3.4.4.)
ii. If the 70-75% efficacy could be maintained the death rate would be 17/10k. IFR= 0.2% respectively. That version requires the lowest cost and discipline. (3.4.5. and 3.4.6.).
MIX VP ELSE EM Protocol (3.5.) The system and efficacy of Mix VP-ELSE protocol
The very rigid management system of the previous VP protocol, controlling the society by military framework, is not always feasible, since not all the society is able to maintain the necessary severe regulations. The MIX VP protocol offers a more flexible solution for the handling of the crisis. However, we can conclude, that the best solution is the pure VP protocol, (3.4.), even in this mixed protocol, a less severe control is applied for the whole AG ppl in 3.5.1. and 3.5.2. for AG1–3, with the use of ELSE for AG4 (entry =quarantine shift is 5 months), while a less severe control is applied for the whole AG ppl in 3.5.3. and 3.5.4. for AG1–2, with the use of ELSE for AG3-4 (entry =quarantine shift is 6-7 months) as demonstrated in the following four examples (Fig. 3.5.1–3.5.4). The scenario too long.
MIX VP ELSE EM NPI Protocols (3.6)
Here we examined the influence of the gradually increasing (0-20-40-60%) level of the traditional NPI (Table 2.9.1. NPI not military controlled i.e ELSE and 2.9.2.) for the elderly group (AG4) in the combined MIX ELSE VP protocol. These NPIs includes a wide variety of actions, such as wearing of mask and gloves, keeping the distance, disinfection etc. The AG1, AG2 and AG3 are under VPHQ (90% efficacy, entering at 0th mo), while the entering of the AG4 with 85% efficacy happened at the one-third (2.3 mo) as well as at the two-third (3.3 mo) of the HI curve. This model clearly demonstrates the combined effect of the NPI and HI. If the entering happens a month later (2.3 mo vs 3.3 mo) the death rate is significantly reduced. Also, the NPI has a significant effect to decrease the spreading of the virus parallel with the strongestness (0-20-40-60%) of the measures.
MIX VP ELSE EM NPI Protocols (3.7)
In order to limit the time frame of the isolation burden, further fine-tuning simulation demonstrate the combined effect of NPI and HI. In this study, the AG1, AG2 and AG3 are under VPHQ (90% efficacy, entering at 0th mo), while AG4 is under (EM)HQSB80+ protocol with 85% efficacy. The AG4 is entering at 2.3th mo (3.7.1.), 2.8th mo (3.7.2.), and 3.3th mo (3.7.3.), representing the 1/3, 1/2 and 2/3 position of the developing HI curves and the plateau of the HI at 4.3th mo (3.7.4.), 5.3th. mo (3.7.5.). This modell suggest that if the isolation cannot be maintained for months, the entry can take place within two or three months if the NPI continues with a sufficient degree. The reason of this phenomenon is that the entry happens earlier, the less VP will be transferred from the AG4 to the AG1-3, and therefore the death rate will be not significantly higher.
All of the models support the supremacy of the ELSE VP (3.4.) protocol.
During the monitoring of the pandemic, the governments and decision makers should construct a system, composed on various GRADEs. Regarding volunteering, acceptance of obligation, management of nursing homes, etc., the effectiveness of the media, civic forums, opinion polls, surveys and the personal influence of the GP, cooperation between the authorities and the public non-state spheres are important. The politically manageable, socially acceptable most optimal variable solution could be implemented by the combination of the following guidelines:
Grade I: Voluntary bases
The current restrictive environment force the seek of solution for the problems therefore it is suitable for the preparation and implementation of several scenarios or their various combinations. If the ELSE protocol is well prepared, then GRADE I, is recommended, nationwide to be implemented first. In this first grade, the government define the voluntary VPCRH and VPD according to the demand and the possibility of the implementation. The state has offered the possibility, for the members of the society, to join on civic responsibility. For the rest of the non-isolated society the decision makers can apply other NPI, if necessary. If someone wants to connect to VPs later, it is possible after two weeks of rigorously controlled (home) quarantine and after two negative tests.
The voluntary VPD
- receives that special allowance as other VP District members
- is compulsory until the end of the epidemic or the development of the appropriate level of HI
- Strict military control with proper sanction
- Home inspection by military control.
- Food delivery.
If we isolate on a volunteer basis some of the VPs, the outcome of the pandemic situation would be considerably better, proportionally of the number of VP. Probably, the recognition, that whoever stays outside stays in the target range, would be in a multiplied at-risk situation, during the rapid development of the HI being in a hazardous environment. Their own and their relative’s responsibility probably would result to join more VP candidates. Effective, robust communication required.
Grade II: Obligatory bases
The continuation of Grade I with restriction of Grade II. By monitoring the epidemiological parameters and if necessary, for those who are a VP candidate but are unwilling to go to isolation mandatory NPI should be introduced. If the VPCRH or VPD are not sufficient, further mandatory VPHQ and/or VPHQSB should be applied especially in the developing countries.
If the VPCRH and VPD is voluntary and nothing else is mandatory, there is a chance that many, especially those aged 80+, will die. Decision makers will rightly hold for this responsible. However, they will not be held responsible if it is made mandatory, further extending the VPHQ and/or VPHQSB NPIs obligatory for other VP. In that case, they will also stay alive at the end of the epidemic. This will provoke temporary dissatisfaction with the introduction of the obligation in the public, but after successful epidemic management, everyone will be appreciated towards decision makers. Any member of the society, who does not follow the accepted restrictions, liable to catch the infection and risks his or her life. Consequently, every member of the society needs to be made aware of the importance of the rules, because it is their as well as their relatives’ responsibility.
The Age Group over 70 (AG3) and/or 80 years (AG4) the (EM) HQSB could be applied for the whole group instead of the only VP over 80yr, with an early entry (+NPI) or with the determined entry time when the necessary degree of HI is evaluated. In those cases, the AG1-AG2 or AG1–AG3 is under VP protocol, and AG3-4 EMHQBS70+ or AG4 is under EMHQSB80+ protocol would be used.
Rationale of the EMHQSB80+:
- People over the age of 80 form the smallest subpopulation of the society (ppl is around 400/10k), therefore the logistics, including the appropriate time zone or whole day for buses and shops, requires the least resources.
- Furthermore, this population moves less spontaneously outside from home and they are vulnerable even without comorbidities.
- The number of VP is ICU/10k=67/10k in the age 70-79 (AG3) while over age 80 (AG4) this value increases 78/10k.
- In the population of AG1+AG2+AG3 (merging 0-79) results the extremely high value of population (9600/10k), - producing the more rapid development of HI, - is than twenty times more compared to the population of age over 80 (400/10k).
Former U.S. secretary of health declared: “We cannot allow the virus to impose intolerable costs in terms of drug, suicide, and alcohol deaths; forgone health care; and more lost jobs” {*} As a paradigm shift gradually becomes enlightened, this new approach is spreading faster than the virus. The emerging important question is how long social distancing measures and lockdowns can be maintained without major consequences to the economy, society, and mental health. Unpredictable evolutions may ensue, including financial crisis, unrest, civil strife, war, and a meltdown of the social fabric.{*} A one-percentage increase in the unemployment rate increases probability of dying with 6%.{*}
The chances of many children being damaged by not going to school are incredibly clear and therefore the balance of risk is very strongly in favour of children going to school.{*} Closure or not of schools had no measurable direct impact on the number of laboratory confirmed cases in school-aged children in Finland or Sweden.{*} The impact of school closure alone is 2%.{*} The negative effects of closing schools must be weighed against the positive indirect effects it might have on the mitigation of the covid-19 pandemic. Online gaming has seen the emergence of record numbers of players, which has facilitated a boost in revenue for many companies.{*} This is a good news for a tiny segment of the economy in a short term, but not good news for the young generation and the whole society, because in the brain of these youngsters similar patterns like in the brains similar patterns and frontal lobe and frontobasal are morphological changes happen like in the brains of drug addict adults, revealed by Hungarian scientists.{*}, {*} More and more papers envision the dark future.{*}, {*} The US congress has approved progressively more several $trillion for COVID-19 relief{*} and this is going to be continued after the election{*} and independently in the EU, too. Expert opinions urge to lift lockdown, which is going to cause more damage than coronavirus.{*} With fears of a new recession and financial collapse, times like these call for resilient and strong leadership in healthcare, business, government, and wider society.{*} Contrarywise, a declaration has been born to call them for the wisest solution of this escalating turmoilby focusing the protection of the Vulnerable Population. {*}
This what the ELSE offers.
The data suggest that the knock-on effects of the pandemic could be larger than those caused by COVID-19 itself — and that they will linger long after the pandemic has ended. {*}
Neglecting or avoiding the needed care has further direct effects on the health care system. Fewer patients visit emergency rooms.{*} The National Syndromic Surveillance Program found that emergency department visits declined 42% during the early COVID-19 pandemic. Estimating this preliminary data in April from the CDC, the deaths of diabetes were 20–45% and of ischemic heart disease were 6% to 29% higher than the 5-year average.{*} In heart failure patients alone, unemployment is associated with a 50% higher risk of death.{*} Organ donation and transplantation have decreased{*} Disruptions in cancer care increase mortality{*} CIDRAP reported that drug shortages can be a matter of life and death, and some shortages mean that a life-saving drug is not available to U.S. patients at any price.{*} If children are not immunized within the correct age window, there may be whole cohorts of children left unprotected for the rest of their lives. Because of lockdowns and the disruption of health services, a 15% decrease in measles vaccinations could raise the burden of childhood deaths by nearly a quarter of a million in poorer countries.{*} It is hard to find the balance between the priorities to control to COVID-19 and to other high-transmission disease threats in poor countries.{*} Many latent childhood psychic stories begin to erupt, especially in the form of panic disorder, because people are most afraid of fear, which is still yet to be explained, and it is not known when it will have a definitive end. Social isolation and loneliness in older people pose health risk{*} The consequences of the direct and indirect effects, like disruption clinical trials{*} and mostly the disruption of economy should result more death than the virus. People are not able to tolerate the condition that is different and negative from everyday life anymore. The world is facing the most serious public health crisis in generations{*}
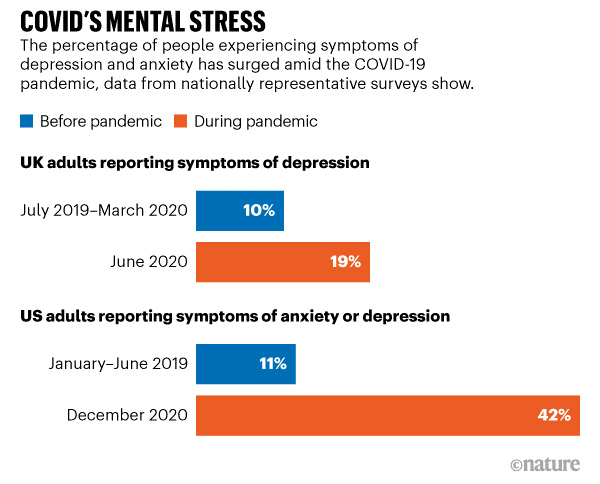
Source: Office for National Statistics (UK data); Centers for Disease Control and Prevention (US data).
Fig. 4.1. Report by the US Census Bureau in December 2021. The symptoms of anxiety or depression increased up to 42. Data from other surveys suggest that the picture is similar worldwide. {*}
The question is how society stands to endure this. Compared to the disintegration of the economy, a much crueler atmosphere of civil war may develop, which is already palpable between the generations, with the working age group urging action with increasingly strong overtones concerning the elderlies, to solve the increasingly intolerable situation. Omens that are even more serious are beginning to emerge in almost all areas of society (e.g. moral, ethical, solidarity, value-based, law-abiding behavior, as well as well-being, mood, health, demonstrations etc.).
Another unforeseen cataclysm would be in the developing countries, where the COVID-19 related health capacity is less than limited.{*} In an uncontrolled outbreak, there is a high risk for the development of a civil war situation at the basis of a socioeconomic crisis and dissatisfaction, and the situation becomes unmanageable on the order of many (ten) millions. If one of the developed countries would implement the ELSE, it could be an example to follow as they realize that there is no point in waiting for the vaccine in the shadow of the new mutants, and no other way to solve the problem except one of the properly applied ELSE variants.
However, if the prototypical execution of ELSE in the advanced-developed world lead to unsuccessful implementation for the reason that irregularity and indiscipline, the under developed- developing word will not adopt the ELSE strategy, concluding it is imperfect, ineffective and thus sentencing tens of millions of people to death. Following the subsequent widespread socioeconomic cataclysm and the resulting global escalation and mass migration would be hard to control by the advanced ones.
This puts emphasis on the importance of the precise military execution. This is not the place of uprepared, untrained civil volunteers. Except if they already have been vaccinated, thus immune protected and also well trained. In conclusion, the ELSE can be used everywhere as GPs for the selection and military staff for the execution can be found all over the world.
According to the author of ELSE, maybe a similar long-term, - difficult to detect or predict - deterioration of the cutting edge of the science can be expected from the harmful effect of the regulations on the scientific era and the training of young scientists. Only in the US, the $55 billion support for university-performed R&D and the student research experiences necessary to train the next generation of scientists is at risk.{*}
Although the emergence of vaccines is a milestone, unfortunately the unprotected nature of the unvaccinated and the breakthrough and/or bypassing nature of the newer and newer mutants necessitate the reintroduction of appropriate restrictions.
The consequences of the related civil resistance are described in and discussed in the 1/A chapter.
Since new mutants assume a herd immunity threshold of 85% or higher, this appears to be unattainable for several reasons.
On the one hand, vaccines are not 100% effective (on average, assume only 90%). On the other hand, a large proportion of (small) children and those under 12 are not allowed to be vaccinated by mothers (cc 10% of the total population). Third, about 10% of the population also refuses to be vaccinated at least. All of this alone is at least 30%, so in the best case, only a herd immune threshold of up to 70% could be developed.
In Manaus, there was a 76% attack rate that resulted in the cessation of deaths in mid-2020, and a few months later in P.1. (Gamma) variant bypassed and/or broke through herd immunity in late 2020 and early 2021 in such an extent that an even worse situation occurred than previously.
It will be of particular interest that Far Easterners, who have hitherto been extremely successful in post-suppression contact tracing, will cope with domestic and foreign opening when, despite the above vaccination parameters, they are unable to achieve a level of herd immunity that provides adequate protection.
Obviously,the the isolation of the unvaccinated or if necessary also the vaccinated Vulnerable Population according to the instructions of the ELSE may provide the most optimal solution for them.
It is worth reviving the experience so far:
The mitigation could slow down the spread of infection but would not completely interrupt its spread, while the suppression could interrupt transmission and reduce case numbers to low levels. However, once these interventions are relaxed, case numbers are predicted to rise proportionally{*}. According to the CIDRAP viewpoint, “the length of the pandemic will likely be 18 to 24 months, as herd immunity gradually develops in the human population until 60% to 70% of the population has been infected. This pandemic will not be over soon, and those people need to be prepared for possible periodic resurgences of disease over the next 2 years. States should plan for the worst-case scenario that includes a second larger wave in fall or winter and one or more smaller waves in 2021. This pattern will require the reinstitution of mitigation measures in fall, in an attempt to drive down spread of infection and prevent healthcare systems from being overwhelmed. This pattern is similar to what was seen with the 1918-19 pandemic.”{*}
The result of the combined strategy could have been bearable for socio-economic life and result in significantly less death, but the prerequisite for this strategy is that suppression have to produce an acceptable low number of new cases for an effective, achievable contact tracing. That is happening in South Chorea, China, Taiwan, Hong Kong and Singapore.{*} The secret to success is the application of ticketing. During the quarantine hotel and /or abundant supply is provided. If the infected person breaks the quarantine the state ensures the continuity even with imprisonment. Maybe the best example of the nationwide testing is Urugay with less than hundred death.{*} After the suppression, the contact tracing was tried to introduce in Germany too,{*} but the early lift faded the aim of the original intention. Although a lot of countries have reached this situation by the end of April, and intriguingly they did not continue with a sufficient contact tracing.{*}
This is especially interesting, since recent paper so apparently summarizes the practical and situational application of the effective combination of the available various NPIs, that it can consider currently the most useful and recommended guide for public officers. As an innovative example the systematically continual use of rapid test – that cost $1{*} and scan a QR code before entering any community, we could immediately know everybody that is infected and isolate these people, reducing R0 about 1, and leaving everybody else mind their business.{*} The possibility of this approach is supported by study of mobility network models.{*} By this autumn the opportunity has gone. Some countries have chosen to lift restrictions when they have more new infections than they had when they decided to impose the restrictions. Even for an expert, it was hard to understand the rationale.{*}
Even though “It is not at all certain that suppression will succeed long term; no public health intervention with such disruptive effects on society has been previously attempted for such a long duration of time. How populations and societies will respond remains unclear”.{*} Justifying this statement, polls show that the economy is starting to take priority over lives, and decision-makers tend to adapt to the Swedish model under the increasing public pressure.{*} Since the unmanageably aggravated damage to all aspects of life, more and more signs point in the direction that under the public pressure, the policy makers would increasingly cast their vote instead more lift, not intensify again the preventive restrictions, resulting the increasing mortality within the VP. Therefore, guided by equal moral respect, fairness, and the importance of reducing suffering{*} the wisest decision would be to start the reparatory works of the ELSE strategy right now.
This is more important with the introducing of the new vaccines.
The real solution has been emerging and more and more opinion has been focusing on the protection of the elderly subpopulation.{*} In the absence of interventions, COVID-19 would have resulted in 40 million deaths globally this year. Mitigation strategies focusing on shielding the elderly and slowing, but not interrupting transmission could reduce this burden by half, saving 20 million lives, but the prediction is that even in this scenario, health systems in all countries will be quickly overwhelmed.{*} Nonetheless, if the society can not tolerate any more the interventions, the whole efforts, sacrifices, devastations up to then would be in vain and the final scenario would lead again to the predetermined 40 million deaths. "This damn virus is going to keep going until it infects everybody it possibly can. It surely will not slow down until it hits 60 to 70% of the population, the number that would create herd immunity and halt the spread of the virus. The big peak is really going to do us in. As much pain, suffering, death, and economic disruption we’ve had, there’s been 5 to 20% of the people infected. That’s a long way to get to 60 to 70%."{*}
The uninterrupting period should be maintained until the development of vaccine. Five-billion vaccine ampoule should be manufactured, distributed all over the word – if possible free - to reach the level of herd immunity, in order to eradicate the SARS-Co-V-2 virus. The present compliance to be vaccinated can estimate about max. 20-30% worldwide or less. In China, for example the Influenza Vaccine Rate is 4 %. (4.6.1.-2.) From these estimations of compliance and immunosenescence up to 20- 30 million deaths can predicted, even the foreseen presence of vaccine.{*}
The compliance is expected to decrease significantly further through media stream, where individual side effects of vaccination reach the “target audience” by magnifying their significance. Characteristic the report of the initial vaccination against COVID-19 which contain otherwise correct information - that the skeptical humble person is unable to evaluate the news with a scientific approach, but perceives that they have only just begun the inoculation and the serious side effects immediately appeared.{*}
As we learn more about the virus, we are developing new ways to protect the vulnerable population, including the elderly, and ensure Americans can seek needed health care.{*} Top epidemiological centers suppose that the success is premised on the ability to keep the vulnerable old and other age groups separated{*} focusing on a much smaller portion of the population would allow most of society to return to life as usual and perhaps prevent vast segments of the economy from collapsing.{*}
The question raises, whether it is possible to design a response that protects the most vulnerable, while simultaneously reopening most of the economy for others.{*} The answer for this question: yes, it is possible.
The COVID-19 attacks a subpopulation that is more specific than ever before in terms of mortality and can be identified by individuals personally, based on age and disease status. They are comorbid patients, the vast majority over sixty years of age who are twenty times more likely to load congested intensive and ventilator machine capacity and die from the virus than the lower age groups combined. With the safe isolation of this Vulnerable Population, immediately after the implementation of the ELSE strategy, life will gradually return to its normal bed, capacity overload will be resolved by isolating the Vulnerable Population - who would occupy 98% of intensive beds and ventilators - and will have plenty of capacity for the 2% of occurring cases. Not only the 20 million lives, spared by the mitigation strategies, but the ELSE strategy can almost save the majority of the 40 million population.
The conceptual confusion that has developed so far is particularly misleading as the so-called "HI strategy". For those who have conceptual misinterpretation in this regard, the author would like to clarify that the vaccine concept is also based on the "HI strategy”.
The goal is to achieve adequate HI level through either natural and vaccine induced immunity. But if the goal is also to eradicate this particular virus, we must use the well-planned combined method.
This became more important with the fast spreading, more contagious new mutant from UK with significantly elevated R0 (probable far above 3) with the correspondingly elevated HI level. By the estimation of the US top epidemiological public officer (Fauci) it can reach the 85%.{*}
The virus will spread further with the Re = 1.5 until the “85%” HI, which could be another year intervallum with several resurgence and about 12-25/10k death in every wave. (Table 1/A/1)
Natural immunity compared to vaccine-generated herd immunity considered to provide more effective, robust protection for the population.{*} Natural infection with SARS-CoV-2 will produce different antibodies. These antibodies can bind to not just the spike, but also to other viral proteins such as the nucleocapsid. Current vaccines in development do not lead to antibodies against the nucleocapsid protein except one.{*}, {*}, {*}
However, among the rapidly evolving data suggesting that as population-wide natural immunity rises, a steady trickle of immune-evading mutations could help SARS-CoV-2 to establish itself permanently, potentially causing mostly mild symptoms when it infects individuals who have some residual immunity from a previous infection leading to be a common, cold-causing coronavirus. Furthermore, also among the rapidly developing vaccine worrisome mutations could also become more common if antibody therapies are not used wisely — if people with COVID-19 receive one antibody, which could be thwarted by a single viral mutation, for example. Cocktails of monoclonal antibodies, each of which can recognize multiple regions of the spike protein, might lessen the odds that such a mutation will be favoured through natural selection, proving the body’s natural immune response supremacy they tend to elicit a range of antibodies.
Since the first declaration of CIDRAP{*} more and more professional leading centers also assumes the development of natural herd immunity. According to expert opinion, counting on a vaccine is not a realistic strategy; the only solution is to build immunity. Protecting the VP and the reopening of schools would be useful in the long-term, as it would allow the infection rate to rise.{*}
The original concept of the UK and{*} Netherlands{*} were based on the protection of natural immunity but the lack of ventilators forced them to put measures in action. The British government has denied that herd immunity was ever its strategy, though a senior adviser to the British government warned them in April that the UK should consider it.{*} Intriguing why the president of the UK, who underwent an obvious infection and is surrounded by the third of the world’s top epidemiologists should be quarantined for just meeting an infected person. Suggesting that re-infection exists, blurring a clear understanding and undermine natural and vaccine induced HI strategy in the eyes of the public.
At the population level, if antibodies cannot be viewed as an indication of immunity, then this undermines the whole rationale for developing a vaccine,{*} or using a convalescent serum,{*} convalescent milk,{*} not mentioning the fate of the Homo sapiens sapiens. Fortunately, the more important role of T cell adaptive immunity has been evidently proved, as it is detailed especially in the introduction. As a living evidence, in the meantime the Herd Immunity against SARS-CoV-2 has been developed in the former hot spots studied in New York City,{*} Italy{*} and Manaus, Brazil.{*} and creeping up in certain crowded areas of the metropolitans.
Intriguingly, now that vaccines are available, everyone agrees that either on a naturally aquired or vaccine induced way the goal is to achieve the right level of protection to provide HI.
During and after the previous waves, the humble and obeying citizen, when the restrictions are completely removed, endured the first shock and rebuilded his little existence but when it is annihilated again and again they give up and no longer believe in decision makers. This could escalate to an unmanageable global crisis with the introduction of the vaccine, the last hope for this social stratum will be dashed if the problem does not begin to be resolved on the basis of clear signs within a foreseeable time i.e. within a couple of months. Especially if the epidemic situation, mortality gets even worse with the introduction of the vaccine.
This further justify that for the vaccine-rejecting VP should be offered the possibility of isolation through VPCRH.
The Swedish model stood up with enough wisdom for this inevitable situation. Mortality ratio is the same as in countries with intermittent austerity, but people have a much more liberated, predictable and liveable burden to bear. These restrictions do not mean draconian tightening one day to another. Therefore, it seems to be that Andreas Tegnell leads his nation in the most proper way and he is veracious in a long term. He acts not only as an outstanding professional, but also as a relevant, responsible public official armed with a wise, calm, holistic approach and strategy.{*}
By the evidences have been accumulated, other responsible, recognized scientists expressed their opinions regarding the most optimal solution, which is the same as the guiding principles of ELSE.{*}
Through Mother Nature, the history of pandemics, the human race always generated natural herd immunity recently together with vaccines. The proof is that we are still alive.
Opponents of the natural development of Herd Immunity suggest that it is not possible to know what subsequent complications of the virus may occur even after a seemingly complete recovery, therefore, we have to wait for the vaccine that will solve every problem for everybody, except those millions who would be sentenced to death during this waiting time. This article has a different point of view. We do not have to wait years, sacrifice millions of lives, and collapse our socioeconomic system, because the related studies suggest similar pathophysiological outcomes as the previous SARS-COV-1, MERS.
According to the review,{*} comprising 94 studies, the SARS-CoV-1 coronavirus targeted in the same way the epithelial cells of the respiratory tract, as SARS_CoV-2resulting in diffuse alveolar damage. Several organs/cell types could be infected – like in other virus induced viraemia - in the course of the illness, including mucosal cells of the intestines, tubular epithelial cells of the kidneys, neurons of the brain, and several types of immune cells, and certain organs may suffer from indirect injury. The major pathogenic mechanisms include dysregulation of cytokines/chemokines, deficiencies in the innate immune response, direct infection of immune cells, direct viral cytopathic effects, down-regulation of lung protective angiotensin converting enzyme 2, (ACE2) autoimmunity, and genetic factors. It seemed that both abnormal immune responses and injury to immune cells might be key factors in the pathogenesis of that SARS-CoV-1 related disease.
A 15-year follow-up prospective cohort study{*} revealed that the pulmonary interstitial damage and functional decline as a consequence of SARS-CoV-1 infection mostly recovered. No other organs mentioned. The study found that in a selected small number of patients (mean age 56) without control group, no symptom history before, who, after the acute phase had recovered from COVID-19, 87% reported fatigue and dyspnea.{*} Patients with community-acquired pneumonia can also have persistent symptoms, suggesting that these findings may not be exclusive to SARS-CoV-2.{*}
For the time being, there could be up to one billion{*} recovered cases from the SARS-CoV-2 infection, from among except sporadic and not representative observations reveal no late complications. The first anniversary of the first unnoticed cases has already arrived. How long do we have to wait?
The large vessel stroke incidence in the 30-55 and older ages, the pathomechanism and autopsy result was the same in the former and present SARS viruses.{*}, {*}
The finding was similar, in a study, where the difference of l cell tropism, viral replication kinetics, and cell damage profiles of SARS-CoV-2 and SARS-CoV-1 were systematically compared.{*}
The results of the study of the SARS-CoV-2 infected rhesus macaques, which non human primates resemble far more to humans, indicated that the primary SARS-CoV-2 infection could protect from subsequent exposures, and combined with the follow-up virologic, radiological and pathological findings, the monkeys with re-exposure showed no recurrence of COVID- 19, similarly to the infected monkey without rechallenge.{*}, {*}, {*}
Corticosteroid use in subjects with SARS-CoV-2, SARS-CoV-1, and MERS-CoV infections delayed virus clearing and did not convincingly improve survival, reduce hospitalization duration or ICU admission rate and/or use mechanical ventilation,{*} although the effect of dexamethasone is most remarkable among critically ill patients on ventilators.{*}
Newly introduced drug fights against cytokine storm (EXO-CD24, exosomes) in COVID therapy, delivering a protein called CD24 to the lungs seems to be very effective, initial report claims. {*}
During the strategy of repetitive cycles of suppressions, in order to generate herd immunity, young and old people are equally exposed to infection, maybe during years. In the case of elderlies, the consecutive high rate of death, 10 times more comparing the age below and over 60 yr (3 vs 69/10k) and 75 times more comparing the age below and over 50yr (1 vs 75/10k).{*} In addition, this process will take years during the repetitive cycles. In the ELSE strategy only, the young population supposed to be exposed only for a couple of months.
No rationale of those risks of death to be compared with the supposed adverse health consequences, which was not supported by any scientific evidence by SARS-CoV-1 and during the last year by the 760 million infections by SARS-CoV-2. None of the studies mentioned subsequent complications of SARS-CoV-1 or 2 cases that were asymptomatic, mild, or moderate (95,6% of infections Imp. Coll. Report-9). Only from the rest serious cases.
Is it worth sacrificing tens of millions of lives and socioeconomic destruction for learning about the later alledged complications of the virus and waiting for the development of a vaccine, not to mention the fact that for the time being we do not know how much time will pass until one will be beneficial enough?
Since it is about the life of tens of millions, I feel obliged to analyze the arguments of the John Snow Memorandum.{*} Although this is an unusual expression in a scientific article and normally, I would not do it, but at this point I feel oblidged to express my thoughts, not only because the points of view of the memorandum are contrary to the ELSE concept and the majority of the cited articles of the memorandum, but for the sake of those innocent victim lives. In the following, I quote from the article{*} of Dr. Nisreen A. Alwan, which is identical of the memorandum.
“Defining who is vulnerable is complex,”
It seems to be complex but can define those vulnerable with great precision. Two articles cited to prove that it is not possible to isolate the VP. On the contrary! It is more than ironic that those two ones prove that it is possible to isolate the elderly high-risk population.
One is an article by Robert Verity et al, which, together with Imperial College Report-9, serves as the basic data source for ELSE. The IFR=0,9%. (72/10k death rate)
The other, also one of the most important references in ELSE, is a brilliant article Clark et al. from the LSTHM. Deliberately or superficially, Dr Anwal’s article states that “the proportion of vulnerable people constitute as much as 30% of the population in some regions”. However, this number (average 23%) is relating for the population, who do not need even hospitalization!
Those who needs hospitalization only the “high risk population” 4% (!) in this article. This is entirely consistent with the aforementioned article by the Verity et al. from the Imperial College, where 4.4% of the infected population is hospitalized, 1.32% of whom are critical cases, and half of them 0.7% in the intensive care unit die.
So not 30% (3,000/10k) should be isolated, but 0.7% (70/10k). Enormous difference, more than fourty times! The cited two articles, which are intented to prove that potential critical cases cannot be isolated, verify the opposite. They make evident, that such a small proportion of the population can be isolated, justifying the underlying principle of ELSE which furthermore demonstrate the rationale of the professional selection criteria of those 0,7% (not 30%) Vulnerable Population.
For the sake of better understanding: If we isolate and protect them, we save their lives. If we do not isolate and do not protect their lives, they will die. So simple.
Independently of their isolation, the necessary measures, intervention, social distance and other NPI regulation can continue if the decision makers and the public consider it necessary, until the arriving of the safe vaccine. Never mind, the whole society (with school closure, economy closure) can wait for the vaccine, in order to save those youngsters (consisting less than 1% of the ppl) from the three weeks of the so-called “long COVID”.
Tremendous responsibility it entails by deceiving the excellence of scientific life by writing 30% instead of 0.7% (which 30% of ppl is really impossible to isolate). Moreover, not referring to the article where the correct numbers are clearly defined. It is pronounced that only 4% are in need of hospitalization and a 1/3 of those needs of intensive care. With this wrong, misinformed arguments, outstanding scientists are misleading, influencing the decision makers in a wrong way, consequently sentencing tens of millions of innocent, vulnerable people to death.
In addition, I assume, the necessary calculations were also not performed when it is declared, that protecting the economy is more effective by maintaining the lockdown in order to protect this tiny portion of the working population from the three weeks of long Covid comparing to the colossal damage caused by the lockdown itself, not only in the economy but also in the entire society.
“Prolonged isolation of large swathes of population is practically impossible and highly unethical. “
The author of ELSE – being also in a high-risk allostatic condition – raise the question: What is higly unethical? To save 40 million similar at-risk people life wordwide?
What does it men “practically impossible”?
This opinion is not a responsible attitude, without the appropriate calculation, the logistic, the feasibility plans, that can be found in ELSE. The ELSE intend to isolate the Vulnerable Population and during this isolation period according to the decline or absence of burden on ICU beds and death, the decision-makers can freely apply the necessary restrictive interventions. Those isolated Vulnerable Population will certainly no longer die. Because they are isolated. They will spend the time in their splendid isolation, regardless of the above-mentioned interventions. No ethical question will raise. Based on the above reasons, it is hard to imagine counterarguments against ELSE. The VP remain in the isolation until the development of a safe vaccine or Herd Immunity, which provides an adequate level of protective shield, when they can return to a safe environment. Of course at that time they would be vaccinated, too. An adequate level means that HI = 58% corresponding to the original R0 = 2.4. With the current constraints, Re = 1.2 corresponds to HI=17%. If the austerity is over, the virus will resurrect and find everyone who has not until 58% HI develops. If the actual Re would shift to a higher level, or to the R0 the HI will be correspondingly higher.{*}, {*} Otherwise, the virus will find everybody and kill those who are predicted, if not this year the next year or maybe ten years later if this prolonged strategy will continue.
The ELSE systematically proves that even 600/10k isolation is possible. That means that the excess buffer of persons in case of IFR=0,9% (72/10k) 9 times, in case of IFR=0.4% (30/10k) 20 times abundant.
“and, like other seasonal coronaviruses, SARS-CoV-2 is capable of re-infecting people who have already had the disease, but the frequency of re-infection is unknown”.{*}
In the quoted article it is written: ”The sensitivity of the RT-PCR tests is variable ranging from 60-80%, hence there is a potential for missing a large number of early asymptomatic cases or those cases where the patient may have recovered but has detectable RNA present, leading to an automatic assumption of re-infection if patients are screened again for a different reason. The RT-PCR tests are also not specific and may detect other corona viruses of no significance. Similarly, another report demonstrated incomplete virus on cell cultures in samples from patients who tested positive post-recovery from COVID-19, again mitigating chances of re-infection”.
Altogether 33 justified reinfection happened from the 90 million infection and the sporadic worldwide up to now below one hundred.{*} All of the 33 cases mutations were intthe background. The patient’s reinfection was differentiated from prolonged PCR positivity after the first infection through whole genome analysis. The two SARS-CoV-2 strains belonged to different clades/lineages with 24 nucleotide differences, which is a high amount given the relatively slow rate of mutation observed for SARS-CoV-2 to date. These clades match the epidemiology of the main clades circulating where the patient was likely infected (i.e. the first strain clustered with viruses from Hong Kong while the second strain clustered with viruses from Spain). Viral culture for the second episode was pending at the time of publication.{*}
Recently published a study with more hypothesis than evidences conclude that 44/6600 participants (0,6%) considered “possible”. 2 of these 44 cases have passed more stringent tests to be classified as ‘probable’ (0,03%). The real data should be consequently less. For the time being, the team does not have enough data to tease out who might be most at risk of reinfection. Recognized immunologist Kassiotis at the Francis Crick Institute notes that participants in the study were mainly women, and mostly under the age of 60. “This group is unlikely to experience the most severe form of COVID-19,” he says, “and may not be representative of the population as a whole.”{*} This can actually happen among youngsters without death, meaning there is no danger of overwhelming the health care system and garden of remembrance. However this study leads to misinterpretations in the common press that immunization lasts only for 5 months and the reinfection 17% etc., which makes the already vaccine reluctant population even more noncompliant to accept the vaccine since the immunity is temporary.
Recent studies prove further evidences of the T cell based present and earlier harmless coronaviruses evoked protection against the SARS-CoV-2,{*}, {*} suggested the Harvard Group’s previous presumption about the possible existence of several combination cross immunity including such a theoretical combination which can lead the eradication of this coronavirus which from this point can consider novel at all. Even mild degree of cross protective coronavirus natural immunity could reduc the transmission dynamic and if immunity to SARS-CoV-2 is permanent, the virus could disappear.{*}
“Uncontrolled transmission in younger people risks significant morbidity and mortality across the whole population”.
The controlled has the same result, just prolonged. The question arises, what is the difference in significancy of the young individuals who recovered after a three-week dizziness and the Elderly who died. I am probably not alone, if I personally would choose the inconvenient three weeks and living further, comparing to death.
“It is unclear how long protective immunity lasts.{*}
Incidentally, the article quoted itself does not prove this: “Our study also has some limitations. First, we only included a small number of recovered COVID-19 patients and did not have the deceased COVID-19 patients..” The quoted article evaluate only the humoral responses.
More and more evidences have been accumulated proving the existence of long-lasting immunity based on T cells response, detailed in the Introduction. By the way, independently the duration of immunity, even “it is unclear”, how can it be an objection against the isolation of vulnerable population? If it is “unclear” that means a further justification of ELSE strategy.
Although the willingness to be vaccinated against COVID-19 is much better than in the case of influenza, it is worth reviewing the statistics so far, because if you are forced to vaccinate again, for example because of mutants this could be a guide:
In the EU, the aggregate influenza vaccination rate has been 41.8% {*} 38% in the US.{*}, {*} 95% of influenza doses are used in the Americas, Europe, and western Pacific; the remaining 5% in Africa, eastern Mediterranean, and southeastern Asia, which collectively make up 48.5% of our global population.{*} In other words, - because 100 % of the doses are far less than 7,6 billion, the entire population, - more than 3 billion people do not get vaccinated from influenza and / or reluctant to get it.
Results of studies concerning these regions indicate that strong recommendations appear insufficient, and that fully funded immunization programs together with high awareness in the population are key to encouraging high influenza vaccination coverage. These programs take years.{*}
Over the age of 65, the influenza vaccination rate is between 10%-34% in the following countries: Austria, Estonia, Germany, Hungary, Latvia, Lithuania, Norway, Poland, Romania, Slovak Rep., Slovenia, and Turkey. The rest of the European countries maintained a vaccination rate of 50–60% among elderly people during the 2010/2011 influenza season, with 82% in the Netherlands and 75% in the UK. In the United States, 66.2% of elderly people received seasonal influenza vaccines during the 2012/2013 influenza season. The situation is worse in developing countries. In mainland China, only 4.3% of adults aged ≥60 years reported receiving the influenza vaccine during the 2011/2012 season. The vaccination coverage of those aged >65 years was 10% in Romania, 12% in Poland and 14% in South Africa in the 2005/2006 influenza season.{*}
In the first systematic review (2018) to analyse the factors influencing influenza vaccination behaviour of elderly people the negative beliefs about vaccination was one of the most common reasons for refusal of vaccination. Elderly people feared potential side and adverse effects, painfulness, concern about the undisclosed content of the vaccine, or belief that the vaccine would cause influenza like illness.{*}
The human immune system completely transforms during the first weeks after birth and changes dramatically again in old age. Therefore, a vaccine that is effective in healthy adults may not work well at either the beginning or end of life.{*} In elderly, a Cochrane review confirmed the safety of the influenza vaccine but found no convincing evidence for its effectiveness.{*} The influenza viruses mutate and evolve with time and the virus vaccination elicits poorly adapted B cell responses in elderly. They have less de novo somatic hypermutations in immunoglobulin variable genes and have less adaptability in their antibody responses to influenza.{*} A study on Yellow Fever vaccination of the elderly pointed to dysfunctional antigen-presenting cells and a dearth of antigen-specific CD4+ helper cells as culprits in the low antibody responses of older vaccines.{*}
From the trial of COVID-19, the results that work in healthy young adults may or may not be extrapolatable information to the population with the mortality of elderlies.{*}
Altered immune competence with increasing age, so-called immunosenescence, is the result of changes at multiple levels of the immune system over time. It includes the altered balance of immune cell production in the bone marrow resulting in reduced lymphopoiesis and increased output of myeloid lineage cells that are also functionally compromised. Thymic involution substantially reduces the output of naïve T cells and the TCR repertoire contracts over time. Although loss of circulating naïve B cells is less profound than naïve T cells, reduced BCR repertoire diversity with age is also well recognized. Furthermore, aging is associated with the dysfunction of innate immune cells like neutrophils at sites of infection possibly due to the poorer capacity of the adaptive immune system to reign in over-exuberant inflammatory responses. The ability to generate adaptive immune responses is compromised by dysfunction of antigen-presenting cells and disorganised and fibrotic lymph node architecture. Collectively, these changes prevent appropriate control of the initial inflammatory response and decrease the generation of an efficient and robust adaptive immune response, which requires the production of large number of functional effector T cells and B cells. For all these reasons, protective responses to infection or vaccination tend to be on average lower in many older adults than in the young, but there is enormous inter-individual variation in people owing to the individual variations of genetics and the history of environmental exposures.{*}
Consequently, study consider it unlikely that a conventional vaccine based on young adult responses will be highly effective in COVID-19 prophylaxis for older adults, therefore it should be rigorously applied to everyone else to achieve herd immunity that will indirectly protect the elderly.{*} Because vaccination alone is not sufficient for proper HI to develop (4.4), natural immunity is also required. A necessary concomitant of this is the high transmission dynamics. The main issue is the bottleneck effect of elderly mortality due to the shortage of ICU beds and ventilators. This is further justify the saving the old generation life to isolate them according to ELSE.
It is highly appreciated that the biopharmaceutical industry is placing an extraordinary effort into developing vaccine to SARS-CoV-2. A safe vaccine is definitely needed as soon as possible. For this purpose, the Operation Warp Speed is established which is a public-private partnership to facilitate, at an unprecedented pace, the development, manufacturing, and distribution of COVID-19 countermeasures.{*} About 150 vaccines are under development.{*} There is no guarantee that initial vaccines will have high efficacy.{*}
Safety is a primary goal for vaccines that are given to otherwise healthy people, and there is a risk that vaccination could make subsequent SARS-CoV-2 infection more severe.{*} Sometimes after years after hundreds are vaccinated could see if a fast-tracked vaccine led to problems.{*} The effect is called immune enhancement.{*} In almost all the examples of vaccine-associated enhanced respiratory disease demonstrated in animals for SARS.386, New technology comes with a learning curve, which can have a human price.{*} Several leading vaccine candidates use mild viruses as delivery systems. But if people have been exposed to these mild viruses in the past, their immune systems might attack the delivery system itself. This could nullify the effect of the vaccine.{*}
There is no reason for rush, because more promisable vaccine development can be foreseen. These antibodies have few somatic mutations, and crystal structures of two neutralizing antibodies bound to the RBD show that mostly germline-encoded residues are involved in binding. The minimal affinity maturation and high potency of these antibodies is promising for vaccine design.{*}
The author is familiar in the area of clinical trials. On the one hand, he had the opportunity as a Fulbright scolar observing such trials in the MD Anderson in the US and participating as a coordinator in an Austro-Hungarian clinical trial. He also closely monitors the potential for rapid drug development because he is also at the forefront of developing a similarly globally demanding pharmaceutical to prevent the long-term biological damage of nuclear disasters like Chernobyl, Fukushima etc. In addition to iodine, the harmful effect of the other isotope, Stroncium90, - which is also actively accumulating in the body, replacing Calcium in the bone, - can be protected by this pharmaceutical to be developed.{*}
The mutation is another factor that has to be taken into account.{*} Most SARS-CoV-2 vaccine developers are targeting the spike glycoprotein which is capable of evading the human immune response.{*}, {*} A uniform mutation occurrence along branches of the A and B haplogroups could complicate the design of future vaccines.{*}
If we are forced to the rapid, accelerated method, the possibility of error is higher.{*}, {*}
The ELSE provides an opportunity to develop the vaccine without any pressure, in a calm traditional way, leading to a widely accepted FDA- approval and trust in the safe vaccine.{*}, {*}
The head of the CDC had told lawmakers it could be fall 2021 before there are sufficient vaccine stocks to allow normal life to resume.{*}
England's chief medical officer has warned it is unlikely there will be an "effective and safe" coronavirus vaccine before the winter of 2021.{*}
It is worth considering, how many times Anthony Fauci, the head of the National Institutes of Allergy and Infectious Disease, and who has advised six presidents, starting with Ronald Reagan during the HIV epidemic, talked, and what he said, about the feasibility and expected timing of effective vaccination against SARS-CoV-2 regarding. The person and the position have synergistic impact. Fauci has since taken opportunities to warn against a forced acceleration of developing vaccine.{*} While the FDA has ways to speed projects, any move to skip the collection of scientific evidence and give an unproven vaccine to healthy people could easily backfire. “You do that in areas where there is an active infection, so you are really talking a year, a year and half, before you know something works,” Fauci said to of the Journal of JAMA. However, that “will involve dosing hundreds or thousands of people in regions at risk of infection, hit hardest by the virus, at the core of an outbreak in areas where there is an active infection, which takes a year, a year and half, before some relevant information would turn up.” Fauci cautioned about what could occur if you “get what you think is a vaccine, and just give it to people. Because vaccine recipients are healthy, there is not much margin for error. So, we are not going to have a vaccine in the immediate future, which tells us we have to reply on the public measures. What is more, despite the fast start, any vaccine needs to prove that it’s safe and that it protects people from infection.” Those steps are what lock in the inconvenient 18-month timeline Fauci cited.{*}
The research teams related vaccine development keeps announcing optimistic forecasts, reaching the majority of readers while so many experts are skeptical about even an 18-month timeline. Opinion suggests that because it is not just the public listening, it is investors too. “They’re writing this for their shareholders, not for the purposes of public health.”{*}
The idea of genetic vaccines is 30 years old. The mRNA is not very stable and can break down inside the body.{*} No one can guarantee that mRNA vaccines will absolutely work. It is not going to happen in a couple of months. It is a promising but unproven modality.{*}
Options can shorten the timeline of the conventional trials of vaccine development of SARS-CoV-2 resulting permission to not earlier than 2028.{*} By the fast-track development it could take 12 to 18 months, and even then, “this is very optimistic and of relatively low probability”.{*}, {*}
Controlled Human Challenge Trials (HCT) of SARS-CoV-2 vaccine candidates could accelerate the testing and potential rollout of efficacious vaccines. By replacing conventional Phase 3 testing of vaccine candidates, such trials may subtract many months from the licensure process, making efficacious vaccines available more quickly.{*} Acceleration of that standard process is necessary.{*} The proposal has gained momentum, 35 members of the House of Representatives wrote to the FDA, and HHS arguing such trials should be allowed.{*} A website has been set up to encourage people to volunteer to be in human challenge trials {*} The FDA regulates every step of the HCT more meticulously, since it involves deliberately infecting people. The first step is the Human Challenge Model before the HCT. Currently there is no challenge model for COVID-19. Developing the human challenge model itself before HCT, could take between 18 months and two years.{*} Researchers have to identify and grow supplies of a strain of the virus to be used in the challenges in a biosecurity level laboratory-3 (BSL-3), that alone takes six months. Once the challenge strain is approved, dosing studies would need to be conducted to determine how much virus to expose volunteers to in the actual vaccine trials. Because of the danger, the researchers would have to start with low doses and work their way up, a process that would take other months. Another time-consuming bottleneck could be foreseen in sustaining the BSL-3 because of the shortage of protective gear and the trainings.{*} After settings, the model the following big steps will be the HCT, which can have the same timelines as conventional trials and in addition, raises ethical questions.{*} A scientist who works for a contract research organization that conducts challenge studies estimated the timeline at 12 to 18 months. Volunteers in the trials would need to be exposed to enough of the virus to develop detectable illness. Between the endpoints have to find the balance.{*} Developing a COVID-19 challenge model may take a long time. Following this, the results from HCT do not always match results from field studies. HCTs may also prove less effective than clinical trials for monitoring potential adverse effects from the vaccine. In that case, vaccine enhanced disease occurring on a similar timeline for SARS -CoV-2 vaccines would arise outside the bounds of an HCT, rendering them ineffective for monitoring such adverse events.{*}
Supporters of the challenge model believe the model could be established in between three to six months.{*} Submission for licensure could occur earlier with a controlled human challenge trial, which will take about three months.{*} Summarizing, the shortest possible time for HCT is six months for the model, twelve months for the trials, six-twelve months of manufacturing and distribution. For the time being, there is only one{*} sign of starting the model.
In addition, only 10 % of drugs that enter clinical trials are ever approved by the FDA.{*} “While the FDA is committed to help expedite this work, we will not cut corners in our decision-making.”{*} The FDA is reluctant of issuing emergency use authorizations to allow for the widespread early deployment of COVID-19 vaccines.{*}
After the bottleneck caused by the shortage of ventilators, a similar one will be emerging by the shortage of capacity of vaccine manufacturing. Countries must line up to access the winning vaccine. If this happens to be in the US, then the rest of the word will have to wait for the first half billion people (US and allied one year) to be supplied and then meet the billions of needs. This will not happen within the next year.{*} Another critical aspect of the spreading of vaccine is to identify groups that should be prioritized for a justified global allocation. The preliminary guidance of WHO, will need more time-consuming detail before its recommendations can become actionable.{*}
Furthermore, even if the word would overcome the previous difficulties the delivering billions of doses of vaccine to the entire world efficiently will involve hugely complex logistical and programmatic obstacles all the way along the supply chain and necessitate more than 8 million cargo aircraft.{*} That means the only the delivery to the airports. The distribution required, temperature-controlled facilities and equipment, availability of staff trained to handle time- and temperature-sensitive vaccines, robust monitoring capabilities to ensure the integrity of the vaccines is maintained. Vaccines will be highly valuable commodities. Arrangements must be in place to keep ensure that shipments remain secure from tampering and theft. Working effectively with health and customs authorities will, therefore, be essential to ensure timely regulatory approvals, adequate security measures, appropriate handling and customs clearance. “Once again, I’m not very fond of easy solutions to complex problems and to believe that once the vaccine is here, we can go back and live as we always have done. I think that’s a dangerous message to send because it’s not going to be that easy.”{*}
Today after December 2, we know the timeline. The new vaccine was adopted within a half year - year earlier than predicted by the most prestigious experts up to a few months ago.
The question still arises, what is real timeline when the (safe and effective) vaccine will work or more importantly will create a satisfactory protective level of Herd Immunity in the entire population? By that time, the estimated deaths could be between ten to twenty million worldwide.{*}
Genetic background.
In the animal reservoir, some of the common ancestor viruses through a large number of mutational series gained a special genetic peculiarity which made them capable as a B1 genome for the spillover - identified by the new host as SARS-CoV-2 - and moreover, together with the further mutant haplotype for the pandemic too.{*} This peculiarity in genetic level means that the SARS-CoV-2 S glycoprotein harbors a furin cleavage site at the boundary between the S1/S2 subunits, which is processed during biogenesis and sets this virus apart from SARS-CoV-1 and other SARS-related CoVs.{*} This polybasic furin cleavage site was found in all SARS-CoV-2 genomes with only two substitutions in two different genomes, belonging to different haplogroups. This segment is therefore highly mutationally stable.{*} A recent study discovered SARS-CoV-2 haplotypes representing > 1/3 of the total (>4,700) database that played a fundamental role as super-spreaders of COVID-19 disease. These haplotypes have three differential features: they reached high to moderate frequencies in the population, they are characteristic of specific continental regions or even individual countries, and they appeared in a very short time period of only a few days. Multiple bottleneck episodes, most likely associated with super-spreader hosts, explain COVID-19 pandemic largely.
The high incidence of a few lineages outside Asia was more probably due to drift and not selective advantages as the subclade A2a. Super-spreader hosts were probably the main responsible for genetic drift episodes and the consecutive multiple bottleneck episodes, which explain COVID-19 pandemic largely. The >160 sub-branches of the two main macrohaplogroups, A and B representing virus strains of variable geographical origins worldwide, is revealing a uniform mutation occurrence along branches that could complicate the design of future vaccines.
Furthermore, arise a maybe more significant threatening potential problem. If the suppression cycling continues for a long time, multiply the chance of mutation during this surveillance period.
This new study on the RNA sequences also reveals that the A2a strain of the virus has altered its spike protein. The A2a strain originating from the O strain is more efficient in infecting humans. In the earlier strains, the spike protein was the key to binding with the ACE2 receptors on the host cells that granted entry to the virus into the lung cells. In the A2a, the spike protein is altered so that it can bind the ACE2 receptors more easily and thus allows it to gain easier access to the lung cells. The reason behind the emergence of the pandemic can be the easy infection capability of the A2a strain. Such mutant viruses increase the transmission and sometimes completely replace the original type of the virus. The SARS-CoV-2 is doing just that.{*}
A SARS-CoV-2 variant with a mutation of Spike G614 has replaced D614 as the dominant pandemic form.{*} G614 is associated with higher viral loads in patients.{*} Further study from the second wave show that all strains have a G614 replacement in the spike protein, a polymorphism that has been linked to increased transmission and infectivity. Patients infected with the G614 variant had significantly higher virus loads in the nasopharynx. Nevertheless, the study showed no indication that the mutation is any more deadly than the D614. Outcomes remain primarily linked to pre-existing conditions such as diabetes and obesity.{*} Other study shows evidence for the increased transmission dynamic for the D614G.{*} As an interesting genetic research finding show that the risk is conferred by a genomic segment is inherited from Neanderthals and is carried by ~50% of people in South Asia and ~16% of people in Europe today.{*} Recently in Uk appeared a new variant.{*}
Over time, we give a chance to develop a mutant nonetheless which may be superimposed on gene-based vaccines and the fast-tracking the timeline meets the messiness of real life: What if a promising vaccine actually makes it easier to catch the virus, or makes the disease worse after someone’s infected? A process called vaccine-induced enhancement, in which the body reacts unexpectedly and makes the disease more dangerous.{*}
Among the rapidly developing vaccine, worrisome mutations could also become more common if antibody therapies are not used wisely if people with COVID-19 receive one antibody, which could be thwarted by a single viral mutation, for example.{*}
A systematic review from ECD about the SARS-Cov-2 reinfection concludes that „the virus isolates in the described reinfection cases were confirmed to house different mutations, confirming infections with new virus variants in the patients. The number of mutations as well as the positions of the mutations in the genome might help to understand the possibility of reinfections and possible immune response escape. Investigations should also analyse the possibility of common mutations in the viral genomes from re-infected patients that could explain the virus’s ability to re-infect. Furthermore, the level of divergence that a SARS-CoV-2 isolate needs in order to be able to reinfect a previously infected person needs to be understood. The role of cellular immunity in the prevention of COVID-19 reinfection was not studied in the reported cases and needs to be investigated.{*}
The ECD revealed 33 cases with a proven mutation in the background until aug 2020. The very rare cases has been following up to now. The frequency not grows.{*} The speed of spread of newest mutant strain from the UK fastest than ever.
Mother Nature always helped the human race effectively overcome the viruses. She can help to eradicate the virus by the herd immunity and if needed through the vaccine boosted excess immunity. We must accept the help instead of challenging Mother Nature to a duel.{*}
Unpredictability and Stochasticity of the Transmission Dynamic in the the onset of the outbreak
Superspreading events (SSE) are characterized by high individual-level variation (i.e. overdispersion) in the distribution of the number of secondary transmissions (i.e., offspring distribution) which means that most cases do not contribute to the expansion of the epidemic, indicated by the dispersion factor (k), in addition to the production number (R). Individual variation and stochasticity play an important role in infection disease outbreak.{*}
In the the onset of the outbreak the initial high overdispersion in the offspring distribution produced by the SSE, resulting an extreme stochasticity and makes the transmission dynamic very unpredictable, where the parameters (R and k) varying in a large scale.
Studies agreed that the SSE representing the 20 % of cases are responsible for 80 % of all transmission (20/80), although a recent sudy suggests as little as 10% of cases could account for 80% of all transmission with the estimation of ranges for R (1.4-12) and k (0.04-0.2).{*} Other studies found lower R and higher k values. Based on data from Hong Kong, the estimated (R) was 0.58 (0.45 – 0.71) and dispersion parameter (k) was 0.45 (0.31 – 0.76).{*} The distribution of individual R values was highly over-dispersed in Shenzen with 80% of infections being caused by 8·9% of cases with R :0·4 ( 0.3–0.5) and k:0·58 (0.35–1.18).{*} Other simulation resulted the R: 2.2 (1.4–3.8) and the dispersion parameter k: 0.54, (0.014–6.95). They estimated the k for SARS-CoV-2 is somewhat higher than for SARS-CoV-1 and MERS{*}
A recent modelling study estimated that the initial basic reproduction number (R0) of the outbreak on the Diamond Princess Cruise ship was 14·8, before any infection control measures had been implemented and while the passengers were a completely naive group.{*}
In a study from 2005 for SARS-CoV, the maximum-likelihood estimation for k was 0.16 (0.11–0.64), indicating a highly overdispersed distribution. According to this analysis, the great majority of SARS cases in Singapore were barely infectious (73% had Re < 1) but a small proportion were highly infectious (6% had Re > 8). Diseases with high individual variation show infrequent but explosive epidemics. This pattern recalls SARS in 2003, for which many settings experienced no epidemic despite unprotected exposure to SARS cases, whereas a few cities suffered explosive outbreaks, which can be explained by the presence or absence of high-overdispersed individuals in the early generations of each outbreak. In contrast, conventional models (with k = 1 or k → ∞) cannot simultaneously generate frequent failed invasions and rapid growth rates. Similarly, the probability of stochastic extinction of an outbreak rises owing to a higher proportion of over dispersed non-transmitting cases.{*} Even with high R0 and no control measures in place, a single case importation is not guaranteed to start a sustained chain of transmission.{*} This is particularly true for infections that exhibit a tendency toward superspreading events, as increasingly reported for COVID-19, but the flipside is, that outbreaks triggered by superspreading are explosive when they do occur.{*}, {*}
This could explain some puzzling aspects of this pandemic, including why the virus did not take off around the world sooner after it emerged in China, and why some very early cases failed to ignite a wider outbreak. If “k” is really 0.1, then most chains of infection die out by themselves and SARS-CoV-2 needs to be introduced into a new country at least four times while being undetected to have an even chance of establishing itself. If the Chinese epidemic was a big fire that sent sparks flying around the world, most of the sparks simply fizzled out.453,
During this period of the onset of the outbreak characterized by the overdispersed offspring distribution hardly obtain evaluable and sufficient data for the trials. Similarly, geographically random outbreaks, where contact tracers have already isolated the infectors by the time participants arrive, make it difficult to obtain data needed for the result.
Human behavior may amplify the potentials of the SSE
The SSE can effectivity be enhanced, and the factor “k” can be reduced significantly not only by virus mutation, but also by human activity by the accelerated mode of transmission with a fast, deep breath and the avoiding of the 3C rules.{*}
A study linked to almost 800 cases revealed that SARS-CoV-2, SARS-CoV-1 and MERS seem especially prone to attacking groups of tightly connected people in closed badly ventilated placed. In addition, the more people in the cluster, the greater the risk. Clusters occurred at nursing homes, ski resorts, churches, restaurants, hospitals, and prisons. Sometimes a single person infects dozens of people, whereas other clusters unfold across several generations of spread, in multiple venues, which indicate a different virulence capability of SSE.{*}
SARS-CoV-2 appears to transmit mostly through droplets and surfaces, but it does occasionally spread through finer aerosols that can stay suspended in the air, enabling one person to infect many. Most published large transmission clusters seem to implicate aerosol transmission.{*}
Difficulties to successfully conduct Phase II- III. trial in the onset of the out break until the development of steady ongoing transmission dynamic of the outbreak
The highly infectious superspreaders and the majority of infected individuals who do not contribute to the expansion of the epidemic cause a highly overdispersed offspring distribution with an extreme stochasticity, which have a potential of serious consequences for the vaccine development. Therefore, it is very difficult to conduct Phase II- Phase III trial in the onset of the outbreak until the steady ongoing dynamic of the outbreak.
In a 20% infector / 80% infectee transmission dynamic environment, the participants will or will not contact due to either a highly contagious ss or a low or not contagious infector. It is difficult to study, identify and isolate superspreaders, because many of them have few or no symptoms and the chance of cooperation is little, because the identification can cause stigmatisation and psycological problems among them. It is also difficult to transport and expose the study participants into the core of an outbreak, which randomly and rarely occurred, in addition, in a short time frame due to the rapid containment by contact tracers. Altogether, these factors may lead to bias in the results of the study.
The new preventive measures aiming toward the elimination of SSE, therefore disease control efforts focus on rapid tracing and quarantine of confirmed contacts. Theoretically, the interest of the conductors of the clinical trials is keeping higher and prolonging contacts between the participants and the SSE, instead of eliminating them. So finally, it could be an intriguing competition between the conductors and contact tracers in hunting the superspreaders for different reasons.
SSE could overwhelm the contact tracing system, leading to the need for broader-scale social distancing interventions.{*} A study similarly - because of the extreme heterogeneity in contacts between individuals and the stochastic nature of transmission, - expect approximately 15% of all primary cases to generate at least one secondary case that is not traced and 10% to generate a secondary case that cannot even be identified. Contact tracing is otherwise of high importance in the early stages to contain spread, and model-based estimates suggest, with an R0 value of 2,5, that about 70% of contacts will have to be successfully traced to control early spread.{*}
Two superspreading, events led to very different outcomes because of the timing and populations involved. One produced rapid spread in a vulnerable population but little onward transmission, while the other was a major contributor to sustained community transmission, including outbreaks in homeless populations, and was exported to several other domestic and international sites. The same two events differed significantly in the number of new mutations seen; raising the possibility that SARS-CoV-2 superspreading might encompass disparate transmission dynamics.{*} Other study observed be the simultaneous circulation of distinct viral haplotypes in metropolitan region.{*}
Important evidence has been accumulating in research about superspreaders so far, which show that most infected people only infect a few other people, but that a few infected people have the potential to infect many more people.456 The evidence of these research can explain the transition from the stochastic onset into the sustainable steady state active predictable classic epidemiological pattern. This paper also points out one of the additional possible explanation of these evidence. Genetic analysis showed that SSE consist of 35% of the population{*} Based on a 20% infector / 80% infectee rate, 15% can be classified as SSE but have less virulence to infect the rest of the population in a small cluster. According to the SSE experts the rest of the 65 % claimed non infector, (Re = zero? among them) but probably this is not the case, otherwise the stochastic phenomenon would be seen in the ongoing stage too. Most probable the Re should be around 1, - among the rest of 65% - and the growing number of those wo has slightly over 1 spread out to a stable ongoing transmission)
After this stochastic onset, the infector/ infectee proportions should change for simple mathematical derivation, therefore, the 65% subpopulation infector role should emerge, and the proportion of stochastic processes reduces. This emerging role proves that the Re for this 65% subpopulation is certainly not zero, but at least 1 or more.
The transmission dynamic in an ongoing steady epidemic for the whole population is defined e.g. R0 = 2.2. Assuming mean R values for the subpopulations, if in case of the remining 65% the Re= 1 then 35% superspreaders should be Re= 6.28. If for 65 % the Re =1.2 then for 35% superspreaders should be R = 4.5 etc. by a simple equation.
After the small cluster period during the onset, the opportunity opens for the growing 65% subpopulation to contribute more and more to a secondary transmission.
This will provide a sufficient opportunity to conduct the trials and minimize the bias in the results of the studies.
Difficulties to conduct Phase II- III. trial in the preventive measures caused low virus environment or since the limited number of infectors
The other crucial fatcor is, that in the present circumstances the preventive measures - contact tracing along with the implementation of physical distancing policies or closures targeting high-risk social exposures such as bars, nightclubs and restaurants - keep the R below 1 the k as low as possible, therefore the outbreak events are rare.{*} In the meantime, more sophisticated and even stochastic preventive models are being born.{*}
Paradoxically, the growing success of efforts to contain the spread of COVID-19 cause an essential problem for the vaccine developers i.e. for Oxford University collaborating with AstraZeneca.{*} How quickly they can reach the numbers required will depend on the levels of virus transmission in the community. If transmission remains high, they can get enough data in a couple of months to see if the vaccine works, but if transmission levels drop, this could take up to 6 months. Recruitment of those who have a higher chance of being exposed to the SARS-CoV-2 virus is being prioritized, such as frontline healthcare workers, frontline support staff and public-facing key workers, in an effort to capture the efficacy data as quickly as possible. A significant proportion of vaccines that are tested in clinical trials do not work. If they were unable to show that the vaccine is protective against the virus, they would review progress, examine alternative approaches, such as using different numbers of doses, and would potentially stop the program.{*}
A Chinese company, CanSino, has also started clinical trials in China using a technology similar to the Oxford institute’s, but demonstrating the effectiveness of a vaccine in China may be difficult because COVID-19 infections dropped substantially.
To determine where to conduct standard large Phase 3 trials could be difficult. If one area drives down its COVID-19 transmission rate, a trial might take a long time to gauge if a vaccine works because there is too little spread of the virus. In places where the risk of getting infected remains high, people may be ordered to avoid as much contact with others as possible or may adopt physical distancing of their own accord. Either reality could drag out the time to an answer.{*}
This happened with Zika virus,{*} where cases have declined to such low levels that Phase 3 field efficacy trials may be infeasible. While great progress was made to rapidly advance several vaccine candidates into Phase 1 and 2 clinical trials, in the absence of sustained viral transmission, it may be difficult to evaluate the effectiveness of ZIKV vaccine candidates by conducting traditional clinical disease endpoint efficacy studies. Pre-licensure clinical trials are typically conducted in areas with sufficient disease transmission.{*} Then raised the possibility of the Human Challenge Trial. Relating this the ethics rules, as a general principle, forbid seeking to infect human test participants with a serious disease. That means the only way to prove that a vaccine works is to inoculate people in a place where the virus is spreading naturally around them.{*}
If social distancing measures or other factors continue to slow the rate of new infections in Britain, the trial might not be able to show that the vaccine makes a difference: Participants who received a placebo might not be infected any more frequently than those who have been given the vaccine. The scientists would have to try again elsewhere, a dilemma that every other vaccine effort will face as well.{*}
All of the others will face the same challenges, including obtaining millions of dollars in funding, persuading regulators to approve human tests, demonstrating a vaccine’s safety and — after all of that — proving its effectiveness in protecting people from the coronavirus. If the pandemic subsides, the trials could be slowed. “That’s why vaccines take such a long time.”{*}
ELSE can provide a predictable, measurable, and uniform background to the Phase II-III. trials. The ongoing 100 vaccine developments require potentially hundreds of thousands of participants in a simultaneous time frame. Current unpredictable epidemic scenarios are not sufficiently met the requirements.
The effects of the SSE and preventive interventions on the Herd Immunity
Superspreaders or individuals who are more susceptible or more exposed are more prone to be infected and become immune earlier, this lowers the herd immunity threshold.{*} According to this idea, in the present strategies, such degrees of overdispersion can be advantageous to disease control efforts if interventions can effectively target the core superspreaders group responsible for the majority of transmission. For example, somehow removing them or achieving herd immunity in this core risk group would have suppressive effects on local transmission more generally. The 20/80 transmission rate corresponds to an adjusted herd immunity threshold of 20%. This compares to a herd-immunity threshold of 60% via natural or vaccine-acquired immunity.
The problem is similar but real with the preventive intervention, because the period when preventive measures affect all mixing rates, proportionally the appearing disease-induced herd immunity level is lower.{*} The more successful a strategy is at temporary suppression, the larger the epidemic is predicted to become later, due to lesser build-up of herd immunity.{*} This arises other problems after relaxing the restrictions. It will turn out, that a lot of individuals remain fully susceptible to infection, because the real herd immunity will be more effective than during the suppression.{*}
With the gradual recovery of HI - with the exception of virgin geographical spots - stochastic cluster phenomena merge into the great mass, losing their significance as experienced during the disaster in China, Italy and in Sweden, where a constant consolidated ongoing transmission dynamic has taken place.
The growing number of protesters against COVID-19 vaccination{*} can result a new excess individuals protected only by indirect herd effects, who remain fully susceptible to infection, should they ever be exposed.{*} They prolong the development of HI, but finally the virus makes justice, because a lot of them cannot avoid it and this way most of those freeriders will contribute to the herd immunity.
A recent Reuters poll found that the hesitancy to take the vaccine would compromise to achieve the required protecting level of herd immunity. „It's not surprising a significant percentage of Americans are not going to take the vaccine because of the terrible messaging, the absence of a communication plan around the vaccine and this very aggressive anti-vaccine movement".{*} Poll from the Associated Press found only about half of Americans say they would get a COVID-19 vaccine.{*}
Trust is the key ingredient in any effort to facilitate a vaccine solution to the current pandemic. Peer-reviewed science transparently assessed in carefully controlled trials by independent experts is the only way to cement that trust. DIY vaccinology is dangerous at a time when nonevidence–based claims of COVID-19 “cures” have done little but sow mistrust of science and public health.{*}
The Economist chart is instructive, showing that trust in science and doctors is inversely proportional to belief in vaccine safety relative to developed vs. underdeveloped countries.{*}, {*}
We have to give a serious probability that the long-awaited vaccine, even in the case of a sufficient ampoule alone, will not be able to protect the entire population and especially the reluctant and immunologically poorly responsive Vulnerable Population. The reluctancy will prevent to build up a sufficient HI level.{*} This again confirms the legitimacy of immediate ELSE, which promotes faster vaccine development.
An additional HI effect that could be achieved through vaccination and the natural immunity generated by infection, together, have several vital importance. This enhanced natural immunity can create probably the only opportunity to eradicate the SARS-CoV-2 virus and not allow itself to continue into a long circulation and to be a possible unmanageable mutant strain. This additional boost to immunization by vaccination could also be valuable on balancing equity, political viability, and the effectiveness of vaccine allocations.{*}
With the introduction of the vaccine, it will not necessarily solve all the accumulated problems promptly. Easy solutions to complex problems are not going to be easy.{*} Mankind is making inconceivable sacrifices in the hope of faith in the vaccine. Although the author considers it ultimately important to have a safe vaccine, we must recognize that the combined effect of antiviral measures and SSE, furthermore the manufacturing and distributing bottleneck together with the FDA process needs time. Experts urge backup plan in place since “so far the story of the vaccine development seems to be that none of the things that could have gone wrong have gone wrong.”{*} Nevertheless, the time of development of vaccine is proportional with the increasing possibility of development of the cataclysm. The ELSE can provide an appropriate environment for vaccine development and offers a prompt altenative solution and the prevention of this disaster.
“It’s impossible to stop the coronavirus. Only Herd Immunity will make that happen. Let’s protect older people, since they are the ones dying.”{*} Let us help to protect older people by using the ELSE strategy combining with the proper vaccines.
Comparison of the protected influenza fatal cases and the unprotected COVID-19 fatal cases
Based on CDC data the vaccine protected fatal influenza cases{*} and not vaccine nor HI protected COVID-19 fatal cases{*} are compared and raises several questions. On the one hand, for the elderly, especially over 70 years, this slight difference will not provide sufficient motivation for COVID-19 vaccination.
On the other hand, how would the figure develop if HI would also protect SARS-CoV-2 – especially elderly – cases, which ELSE VP offers, saving their lives. The results of calculations of averted cases (see the reports of Pitman and coworkers) in this direction tend toward the influenza much more balanced proportions, with the mortality of toddlers being even worse.
The risk Let’s protect older people, since they are the ones dyingof youngsters, (especially 0-4 yr) a magnitude higher with the vaccinated influenza ages than the non-vaccinated COVID-19 cases. Relatively few cases of infants confirmed to have COVID-19 have been reported, those who are infected have experienced mild illness.{*}
IFR for COVID-19: 0,2-0,9%, while IFR for Influenza: 0.01%. ELSE VP can also reduce IFR to 0.06%. Natural and vaccine generated immunity can maintain this level — and it is more likely that it can maintain it at an even lower level — until viral eradication is achieved. This is the same for IFR, COVID-19 will continue to take its toll among the elderly, while the flu will take its toll among children as well.

Fig. 4.6. Relative risk of death from influenza or pneumonia vs. COVID-19 is higher for those under 25, and lower for those over 25. Estimating relative risk is highly dependent upon the ultimate lethality of COVID-19, which is unknown at this time. Nonetheless, a clear pattern emerges from what we know, in which those under aged 25 are at the lowest risk of death from COVID-19, or pneumonia. (Source: A. Roy / FREOPP {*}) relative to influenza.
There is a probability that two-thirds of the world’s population will be reluctant and/or will not have a chance to receive the SARS-COV vaccine. In addition, even if the vaccine is effective in the young, it is unlikely to work effectively in the elderly.
Another problem could be the growing number of protesters against Covid vaccination{*} who could enlighten the elderlies and reduce their already diminished compliance. Elderly compliance will be expected to be similar to that of the flu and they will not vaccinate themselves.
Young people who fear their children for the brand-new vaccine will be even more reluctant to get vaccinated for the other two reasons. On the one hand, because it will be impossible to know who will be protected by the natural way and who will not be, and there will not be enough tests for mass serological surveys to make distinction among them.
On the other hand, the intensifying anti-vaccination campaigns will make them ambivalent, nevertheless the elderlies, too. They could not decide whether a mostly asymptomatic virus or a new type of rapidly developed vaccine will be more dangerous to them.
In addition, they should only be vaccinated after so many ordeals to continue to protect the elderly, who will have the opportunity to finally protect themselves and yet refuse to even vaccinate themselves. Why? The confrontation between the generations will be worsening to the end.
Because of the drastic cuts being introduced, the next wave, together with the flu, one on top of the other can be devastating. Being infected by a flu, which is a burden on the body that drains resources and puts a strain on the immune system, can consider a similar health state as for example being comorbid and subsequently on the top being infected by a Sars-Cov-2 too, the consequences are unpredictable. The younger generation will most likely also be more affected, and the world would face a terrible “ConFluD-21” situation. Almost nothing is known about the interaction between the coronavirus and influenza, experts say. It is possible for someone to be infected with the coronavirus and influenza at the same time, but experts have very little data regarding it.{*}, {*}, {*} Furthermore this could place a tremendous burden on the health care system.” If the first wave of the coronavirus outbreak and flu season had peaked at the same time, “it could have been really, really, really, really difficult in terms of health capacity.”{*}
Health experts are especially worried that a bad flu season could combine with the coronavirus pandemic in fall and winter to overwhelm hospitals. Flu vaccine manufacturers are already making millions of extra doses in a bid to prevent that from happening. “We want to take flu off the table, in every way possible, make flu a non-factor,” the chief strategy officer of the Immunization Action Coalition nonprofit told The Washington Post in the past week in a report about the push. Americans to get a flu vaccine.
Experts in the absence of interventions envision deaths similar to the 1918-19 flu pandemic{*}, which ranged from 50 to 100 million. However, the population of the earth at that time was 1.8 billion, which is now four times that equivalent to 200–400 million deaths. SARS-CoV-2 is four times less dangerous. The probability of SARS-CO-2 mortality is one-fifth, one-tenth of the 1918-19 flu pandemic.
This also suggests that if ventilators shortage were not a bottleneck for the health care system, out of the eight human pandemics in the last 300 years, COVID-19 would not necessarily be classified as severe the COVID-19 among them. Although the original strain became more human-adapted, calculation of the averted flu cases that much more affect the 0-4 age group, the seriousness is still comparable.{*} By precisely implementing the ELSE strategy, up to 98% of deaths can be prevented.
Recent systematic review of the immunology of the COVID-19{*} highlights the significance of the innate mechanism. The natural killer cells{*} enhanced by interferon{*} could play a role among the the first line of defense.
Interferons can both enhance{*} and decline the severity of respiratory viral infections.{*} Recent study demonstrated that patients who received inhaled nebulised interferon beta 1-a (SNG001) had greater odds of improvement and recovered more rapidly from SARS-CoV-2 infection than patients who received placebo. The odds of improvement on the OSCI scale were more than two-fold greater in the SNG001 group than in the placebo group on day 15 or 16 (odds ratio [OR] 2·32 [95% CI 1·07–5·04]; p=0·033; and more than three-fold greater on day 28 (3·15 [1·39–7·14]; p=0·006.{*}
Recent genetic study put emphasis on the possible importance of interferon, too.{*} With severe COVID-19, rare putative loss-of-function gene were identified that were associated with impaired type I and II IFN responses.{*} Excess mutations involved in the regulation in the type I and III IFN pathway that may determine the clinical course of the infection,{*} manifesting autoantibodies to those interferons.{*}
Ethical and legal issues arise regarding to data protection during the selection of patients to the VP, the decision coercion between life and death in the ICUs, compliance with public health regulations, immunity passports, and the adverse health consequences in the population exposed to infection during the generation of herd immunity.
The members of the VP should be identified. The first issue could be the data protection of these patients. In this emergency, data protection advocates should consider how much they would contribute with protecting every person’s data – (making the implementation of ELSE impossible - to increase the public cemetery open data of those, who no longer require protecting their data.
Everybody has the right to the ventillators. That is true and correct. However, representatives of this correct opinion from the desks ought to go to the spot and should be faced with the vital horrific ethical dilemma when the doctors force to decide who is entitled to the ventillator and who dies.{*} The author was faced frequently to similar situations when the ICU was full.
In the ELSE, the Vulnerable Population is assumed for compensation. In a survey, assessing the public compliance rates with self-quarantine and compensation was also assumed, the compliance rate was 94%, yet, when compensation was removed, the compliance rate dropped to less than 57%. That study demonstrates that providing people with assurances for their livelihood during self-quarantine is an important component in compliance with public health regulations.{*}
Regulations should be mandatory, but individuals who resist, should simply be ticketed an amount sufficient to motivate compliance.{*} This may also apply to those who reject to join the Vulnerable Population, (VP) if the number of volunteers is low or the authorities ordered mandatory joining. In addition to the promise of compensatory wages or the threat of fines, the ticket can be supplemented by the fact that rejectors will be obligated to be vaccinated upon arrival of the vaccine. Similarly, if volunteers endanger themselves from altruism in a clinical trial and justify a well-deserved advantage who lacks this community self-giving solidarity, they will be disadvantaged in a similar proportion to the opportunities available.{*} In theory, challenge trials could enroll volunteers who are at low risk of harm from the virus that causes COVID-19–dubbed SARS-CoV-2–such as young adults who rarely develop serious symptoms after becoming infected naturally. Deliberately causing disease in humans is normally abhorrent but asking volunteers to take risks without pressure or coercion is not exploitation but benefitting from altruism. We are aware of multiple offers from people willing to volunteer for the challenge studies.{*}
Before starting ELSE, similarly these volunteers and the soldiers who has to contact with the Vulnerable Population, ought to be protected similarely by the dubbed SARS-CoV-2, causing COVID-19. What kind of ethical question would arise if it were natural for ordinary people that firefighters and front-line health workers are fighting COVID-19 at the risk of their own lives not on a voluntary basis. Furthermore, if, also not on a voluntary basis, the US sacrificed such a number of victims among their young sons, in Vietnam for a questionable war, what kind of ethical issues now arise if they have to protect their parents on a voluntary basis, by an incomparably safer exposure resulting zero death among these young soldiersEthical committee has accepted the “bionic solder” development resulting more serious invasion, implants etc in the human body.{*} Our situation in this pandemic is analogous to war, in which there is a long tradition of volunteers risking their health and lives on dangerous missions for which they understand the risks and are willing to do so in order to help save the lives of others. Every week of delay in the deployment of a vaccine will cost thousands of lives.518 This is true for ELSE ,too.
Immunity passports of the individuals protected by natural immunity could support returning to work, but also face significant technical, legal and ethical challenges.{*} However, they can be a very valuable portion of the population, they could help others, for example health-care, elderly home workers, volunteers with immunity could return to the front lines, others back to work, especially busy enclosed spaces, restarting parts of the economy more quickly and safely not mentioning the ELSE project.{*} How much were important the ethical challenges in the Ebola outbreak in Congo, where survivors played a special role in providing care to people who were sick.{*} After a successful implementation of ELSE VP in the developed country, a strong-handed president will immediately realize its significance and will not argue much with data protectors and ethicists in the underdeveloped regions.
Not much is mentioning by the ethicists about the health care workers who are obliged to risk their own health, witnessing higher rates of death, and experiencing breakdowns of protocol and support. Treating critically ill patients during the pandemic is an enourmous task and the continuous stresses could lead to mental health issues, yet therapeutic support is lacking.{*} At least 1,500 nurses at two hospitals in the Philadelphia area are planning to go on strike.{*}
Furthermore, there are bioethicists who analyze and judge ethical issues with a balance imbued with sufficient wisdom in the interests of the individual and the public good and for example the attracting study{*} participants by offering incentives. Society also let humans volunteer to do risky things all the time, for example, volunteer to be emergency medical services during this period. That significantly elevates their risk of being infected. In clinical trials in general, the focus is on not only reducing risks to participants but achieving a reasonable balance between the added risks that they take and the importance for the community. Vaccines could be our societies’ a way out of the bind between economic stagnation and widespread mortality.{*} This realization led the UK to test vaccines on volunteers deliberately infected with COVID-19.{*} The other way could be the ELSE.
The ethicists – exceptionally in the SARS-CoV-2 caused global situation - should be aware, that not only the moral aspect is the basis of judgment of a complex situation, but also the decisions in policy and practice are guided by three moral values: equal moral respect, fairness, and the importance of reducing suffering.{*} If the importance is the saving millions of lives than this value becomes the most important before everything ELSE.
Skeptics doubt that vulnerable populations could really be protected. For them such superficial explanation like multiple generations live under one roof, young people work at nursing homes and so on are good enough to conclude to the unenforceability of measures to prevent infection. The author did not find a carefully planned, scholarly developed and analyzed study of the safe isolation of the vulnerable population to meet the elementary scientific requirements. The significance of saving those ten million lives would deserve at least one.
It is necessary to analyze the events so far on a broad horizon and to make decisions determining the future because of consensus by the policy makers and experts of the socio-economic life.{*} If policy makers were convinced that ELSE VP was a safe strategy, they would obviously opt for it immediately.
For ELSE, a safe strategy means nothing more than a technical operation conducted with strict discipline. This is a not a theoretical epidemiological but a simple practical logistic task for those designated, eligible, qualified and devoted military recruits and should be implemented in a well structured, highly prioritized, regulated manner.
This study repetitively emphasizes that only military logistic experts capable to evaluate and judge the technical feasibility, therefore the author requests the readers that - except the scientific sections of this article, - leave the declaration of opinion and the decision, regarding the technical feasibility on military logistic experts.
The author consulted on the feasibility of strict quarantine of ELSE with a high-ranking military logistics commander. He summed up the answer that it is a finger exercise. Their regular military exercise is an exponentially more complex task. By the way, he said, what can the nation expect from us if the enemy attacks our country in an incomparably more complicated way if we can not protect this limited number of populations of older years with military discipline, without doubt?
The following suggestion could be an example to follow or adapt by all countries wordwide to establish unified command system.{*} First, need a commander who have the President’s full confidence and must earn the confidence of the American people. This is not a coordinator across agencies. This with a commander carries the full power and authority of the American President to mobilize every civilian and military asset needed to win the war.{*} The first step has been taken place in the US by General Perna, chief of the Operational Warf Speed.{*} Rather than stumble through a series of starts and stops and half-measures on both the health and the economic fronts, we should forge a strategy to defeat the coronavirus and open the way to economic revival.{*}
Defense Secretary Mark T. Esper declared: “I am confident that, as with any mission our military undertakes, we will adapt and overcome all obstacles in our path."{*} This statement together with the President of the United States similarly declared that this is a war of such a magnitude that it cannot be compared to any previous one. Not only human lives, but also the economy was facing regarding the strike.{*} It has never happened in history that the world’s most powerful army should envision full military readiness for a fight without strategy. However, to defeat the enemy can be solved with fragmentary resources through precise disciplined execution of ELSE.
The primary reason for the elaboration in the article with such depth, which goes even into minor details, is that the author is trying to prove that the safe isolation of VP is feasible. With proper, precise design and control no infection can occur. Provided but not allowed, if it does happen, the process to control is much easier than if it happens outside in a diffuse uncontrollable external environment. The Vulnerable Population, like volunteer vaccinators, are closely monitored as in volunteers in HCT.{*} They would also move in small groups in the district in order to tighten the spread of virus make microclusters in the district. The average social distance is 6x6 m. These altogether should minimize the risk of spreading of the infection.
Let it be a living example of Senegal’s disciplined response to a SARS-CoV-2 attack. They would be able to execute the ELSE without any complication, without minimal infection. The VPHQSB efficacy would be not only 85 % but also at least 95%. Why? According to the Global Response{*}, (covering 36 countries, which measures the degree of preparedness and a reliance on facts and science including a mix of wealthy, middle income and developing nations), Senegal ranks 2nd while the US ranks 34th. In Senegal, 16 million, there were 14,000 infected and 284 dead in six months. Comparing the US should be only about the 10 thousand dead.The main reason of this difference is that the US did not have Ebola epidemic experience. This experience during the 2014 Ebola outbreak is still vivid in the Senegalese. This causes the population tremendous discipline to follow everything from the authorities who excellently organize prevention, communication, test and contact tracing. Hotels (!) have been transformed into quarantine units.{*} According to the scientific “experts” of the developed countries it is impossible to quarantine people in hotels, nursing homes etc. Otherwise, a country has a fragile health care system, a shortage of hospital beds and about seven doctors for every 100 000 people.
The ELSE VP starts with voluntary isolation. Volunteers who are aware that it is about their lives will act with similar discipline as Senegalese who have experienced Ebola. It is reasonable to presume that they submit to all instructions in order to defend their own lives. The soldiers will protect the VP from the virus, as if they would be defending their homeland from an enemy.
Why it is possible to implement the isolation of VP safely:
The unique feature of the virus is that it attacks a specially, personally identifiable ppl. the most effective method is currently the safe isolation of these VPs because the availability of a safe effective vaccine can take months or even years.
- If military logistical experts, declare that there is no uncertainty about the possibility of safe isolation, and they are able to follow the guidelines and directions of this article.
- Does it mean that there is no doubt that isolation of ELSE VP is feasible? YES
- If there would be not enough already protected recruits, would it be enough volunteer soldiers to be vaccinated with the virus?
- Is it possible? YES
- Volunteers should be selected (from among US: 100 M EU: million already infected and protected persons) to perform staff duties in ships, resorts, hotels, nursing homes.
- Is it possible? YES
- Transport of VP to sites without infection. Preferably, to the nearest cruiser, resort, hotel, etc.
- Is it possible? YES
- Based on the protocols described, (two weeks of quarantine, tests, etc.) is it possible to ensure that the site is definitely not infected at the beginning?
- Is it possible? YES
- Preventing the virus from penetration by allowing only protected soldiers or protected staff to encounter the outside world and all imported products undergo disinfection.
- Is it possible? YES
If all this happens, the VP can spend their time in sheltered isolation, as a reward as a holiday - for as long as possible - the sunny social order is restored and everyone can do their duty in peace. In addition, there is time and especially opportunity to develop a safe vaccine during the steadily developing HI.
Last year (2021) for the developing countries, i.e. WHO’s Africa chief declared the goal is to vaccinate only 20% of the population on the continent by the end of the year. {*}The goal could not be achieved. That means that throughout 2022 and the next following years the virus will take its victims with millions of death in the developing countries, too. This further justify that for the VP, especially the vaccine-rejecting VP should offer the possibility of isolation through VPCRH.
The first modern pandemic requires innovations vs. the coronavirus.{*}
Isolation of VPs is independent from lifting restrictions of the rest of the population. Decision makers and young generation can decide freely on a consensual basis, according to the epidemiological parameters, the decline or absence of burden on ICU beds and death and the actual progress of vaccination.
Most importantly, those isolated Vulnerable Population will certainly no longer die from COVID-19. Moreover, the direct cost is less – even for a year isolation - than suffering and dying in the intensive care. (2.7.1.) The indirect cost is a fraction of the recoverable colossal amount of money ($10trn) {*} that arises immediately when the social economy is functioning normally, and the GDP’s numbers return.
Natural Herd Immunity boosted by the vaccine may be a current and one-time opportunity for humanity to eradicate the virus. {*} The Homo sapiens sapiens should be able to eradicate SARS-CoV-2 with the combined use of ELSE and the supportive safe vaccine generating the appropriate level of HI. Or at least try to make all possible effort to achieve this goal.
It should be in the framework of a wise broader horizon to use the vaccine, through an internationally agreed and cooperated implementation embedded in an internationally coordinated master plan – incorporating ELSE - in order to eradicate this “challenging” virus forever. The COVAX as an essential element of this plan has to succeed. The trust in responsible leaders is the key ingredient of this master plan to facilitate the most effective solution to the current pandemic. {*}Regardless of the above-mentioned necessary or unnecessary interventions, the VP will spend the time far away in their deserved splendid isolation and consider those lifted interventions like the spooky action at a distance.{*} That mysterious action at a distance through the rapidly evolving scientific knowledge became evident by physical experiment,{*} and it is further pre-contextualizing in living systems by the deciphering of the yet undiscovered significance of the “outside in” phenomenon through the social level network of individuals{*} and the “inside out” by the individual’s internal network.{*} In the current situation, the approach is well articulated in the complex nature of the fight against COVID-19 by the opinion of the chief editor of the Lancet. “The economic crisis that is advancing towards us will not be solved by a drug or a vaccine. Nothing less than national revival is needed. Approaching, COVID-19, as a syndemic, will invite a larger vision. Viewing COVID-19, only as a pandemic, excludes such a broader but necessary prospectus.”{*} The author agrees with this conception and hopes to contribute to these efforts with this book.
For the time being, today, two options remain: “Either we let many of us get the coronavirus, recover and get back to work — while doing our utmost to protect those most vulnerable to being killed by it. Or we shut down for months to try to save everyone everywhere from this virus — no matter their risk profile — and kill many people by other means, kill our economy and maybe kill our future.”{*}
So, let us start saving our beloved ones, our economy, and our future.
Before everything ELSE!
Scientific articles are usually intended for a defined scientific team. The imperative urge to act immediately rarely occurs. However, in the case of SARS-CoV-2, scientifically inspired assumptions and conclusions demand prompt practical action. Nevertheless, the power of science lies in its understanding by others. The ELSE offers a paradigmatically new approach in the fight against this novel virus. To make understandable for decision-makers and, through the qualified journalists and editors, for the wider audience, this approach should be implanted in a comprehensive analysis and systemic review that can unfold from scientific recognition and hypothesis in order to justify the strategic steps that could be the most effective in both the short and long term. The format of a book provides an opportunity to expand and explain an idea or concept of which a few-page essay is not capable.
The author has been working on this article, growing to a book format, since the publication of the Report from the WHO Joint Commission in February 14, 2020. Since then, unprecedented epidemiological research in the field of scientific, technical, and social cooperation has emerged, along with the concomitant rapid progress in vaccine development.
Based on the opinion of the most experienced professionals, even from the head of CDC in September {*}, the author interpreted the cumulative opinion that the earliest date of the authorization of the developing vaccines will be in the middle of 2021, rather than at the end of 2020. {*}, {*}, {*}, {*} This, otherwise extremely important and highly appreciated breakthrough, could create unpredictable turmoil due to the impatience and intensified expectations that "everything will immediately be resolved" by the vaccine and, furthermore, due to the reduced compliance and immunological response of elderlies. {*}, {*} Another novelty is that the new coronavirus mutations could cause more reinfections, raise specter of immune escape and require updated vaccines. {*}, {*}
The main element of this book is that the isolation of the Vulnerable Population (VP) has become more urgent than ever to prevent the almost unmanageable problem that is expected to arise suddenly and unpredictably starting from the beginning of 2021. This is evaluated in the introduction 1/A. Otherwise, the related analysis of the previous time in the discussion (in chapter 4) remains relevant.
In this extremely rapidly evolving epidemiological and consequential socioeconomic scenario, it is necessary to follow events and adapt them to the basic concept. This will be done either on the author's website with a constant interpretation of the most important proceedings and in the publisher L’Harmattan’s website, summarizing larger periods corresponding to the strategy of ELSE.Recommendations to be considered in order to minimize the potential infection in the VPCRH.
- From the abundant number of immune protected persons (within an average of 1/3 until to now of the total population) sufficiently enough people can be rendered for this purpose.
- The resorts are suitable to reduce the possibility of infection due to the separated buildings, which allow gradual saturation by guests.
- In the Cruisers and Hotels, the mandatory operating-rules correspond to the applied protocol must be created. This should be done in such a way so that phase operating rules that are effectively solve the infection isolation.
- For the restaurants, every time people should arrive there at the same time. People must always use the same lift. The lifts must be programmed in order the contact should happen in clusters of small groups. People should arrive punctually at the dining room, where at the beginning there is a matrix-like table distance of 6 * 6 corresponding to SD, etc.
- VPCRH should also have sectional contacts if possible. It will be determined what closed groups can move in stages, segmented together. If there is an infection, then that group needs to be quarantined. Meals of the employment must also take place on a scheduled basis.
- Accordingly the staff of the apparels to be identified staff members. Those who have been through natural means and / or infection by vaccination are considered to be protected in this way, and has been trained for the awareness of any kind of potential infection and for contact tracing should wear a white uniform, even if they need bedside care for other reasons.
- Those who live strictly inside the resort and come into contact with VPs, through their assignment, should wear orange attire. Those who also live inside the resort but do not need to communicate with patients should wear black uniforms. Due to the necessary supplies, only protected military personnel are allowed to contact the outside world.
- Contact Tracers ready to declare if someone develops symptoms, they should immediately follow the protocol developed specifically of that resort. The patient and the other infected will be admitted to hospital. The group of the infected person can be quarantined in a separate building within the resort.
- If possible, VP doctors, and former nurses who are willing to work for some compensation could be selected to be professional staff who perform primary care activities.
- Supplies must first be deposited in a separate room where they are properly disinfected.
The designation of possible districts obviously depends on local characteristics. This is a function of the geographical, labyrinthine logistics, and physical capacity of the patient population for the functional radius of a given area. Municipality and local police can help in the designation.
Table A.2.1. Establishment of districts for the Vulnerable Population (VPD)

The number of patients who can be accommodated in a good atmosphere, which allows for an average of 100 * 100 meters and a distance of 6 meters between individuals, can be accommodated in a strictly isolated area, in a good atmosphere. With the yellow cordon double, /10m/ in the area isolated from outsiders.
Table A.2.2. In the case of districts accommodating 250-350-500 people, the number of possible districts and the capacity.

aNationally available number of people if everyone (500 people) visits the district daily
bNationally available number of people if everyone (500 people) visits the area every third day * 3
cNationally available number of people if 400 people every third day * 3 and if 100 people living in a family house with a garden only every six days * 6 visiting the area
dNationally accommodable if 300 people every third day * 3 and if living in a family house with 200 people only every six days * 6 visiting the area
eNationally accommodating if 300 people every third day * 3, and if you live in a family apartment with 200 people, you only visit the district every twelve days * 12
The number of members of the Defense Forces needed, depends on the number of districs and their task. The Armed Forces will protect the country from any attack, this is their job at present! The current enemy is now uniformed, uniformed little creatures who are attacking our country in an unorthodox way. He rated the outlook as worse than comparing all the US wars. The US president also compared the attack on viruses as a war.
Table A.3. Required staff from the army.
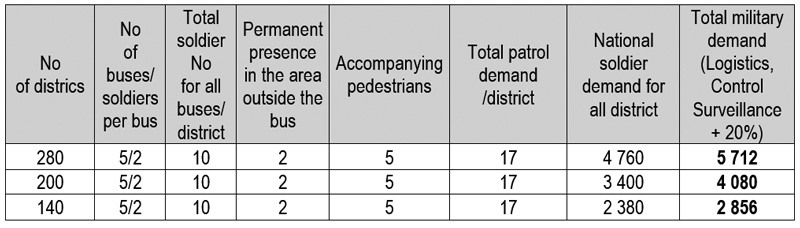
The number of required military personnel is over calculated. There were 5 buses in each district, including two patrols and five infantry escorts. The non-terrain demand above the districts has been calculated at 20%, which is already well above the demand for the largest district number (280). The number required is therefore between three and six thousand/10 million ppl. In Hungary there are currently 40,000 troops available. (25,000 active, 10,000 can be called up within five years and 5,000 reserve) This number is sufficient to supervise and transport up to half a million VP.
- Camera will be placed in front of the entrances of the VP’s apartments, which will take the foreground non-stop. Always look through the previous day to see if there is any movement. This goes fast because the recording only captures the movement. An alternative to Taiwan: The designated handcuff-like transmitter wears a scan of the apartment and when the individual moves out, it gives an emergency alarm or the latest mobile phone application.
- Districts send a daily report to the Operational Staff where a national summary is prepared, which is compared to the current epidemic situation.
- Military personnel serving in the districts must start work in an infected and thus protected state. To this end, after rapid selection, assistance is provided among Covid-19 active infected individuals without a mask. They are tested in every five day. They can go to the districts, when there is no sign of SARS-Co-2 virus, but sign of adequate level of antibody.
Detailed instruction of transport of the VPD
- After and before the local buses have completed the bus service for commuters, between 9-11 and 15-17 (after and before commuting times) the members of the Vulnerable Population are collected and repatriated.
- The most optimal solution is to run special buses (microbuses) on a special route, nonstop every day and keep shops open exclusively for the VP. This means running fewer buses and shops with signicantly less possibility of infection. The isolation of VP more effective than the with the time zone version. The most effective protocol is to use the dedicated buses and shops all day long. 2.9.2. VPHQBS)
- There will be service interruptions on regular flights during the circulation of the directional buses
- All directional buses will be disinfected before departure, in the bus round belonging to the district, where this work is performed professionally by the district hygienists.
- With two escorts per bus, who disinfects the handrails in a short time before each round (everything that passengers are accomplished by hand)
- The attendant supervises them (keeping distance, wearing a mask, etc.) on the road, on the bus to avoid infection
- If the Vulnerable Population member can only travel by elevator, it is advisable for the attendant to get on the elevator and professionally bring them down to the bus waiting at the entrance. Do not touch anything in the elevator (6.9)
- For this reason, two attendants are needed, but this can be solved because those who supervise the outdoor activities are involved in the running on site among the elderly
- Camera will be placed in front of the entrances of the VP’s apartments, which will take the foreground non-stop. Always look through the previous day to see if there is any movement. This goes fast because the recording only captures the movement. An alternative to Taiwan: The designated handcuff-like transmitter wears a scan of the apartment and when the individual moves out, it gives an emergency alarm or the latest mobile phone application.
- Districts send a daily report to the Operational Staff where a national summary is prepared, which is compared to the current epidemic situation.
The transport of the Vulnerable Population.
The main transporters are, of course, directional buses. Anyone who cannot move on foot or is too far away will be transported by military passenger carriers. Between panel houses, military jeeps or minibuses may be more efficient. Routes to outdoor locations should be designated. Positions where the movement of the Vulnerable population can be controlled should be identified. Eg check for unavoidable intersections where the risk of contact with the outside world is increased, paying more attention.
- After and before the local buses have completed the bus service for commuters, between 9-11 and 15-17 (after and before commuting times) the members of the Vulnerable Population are collected and repatriated.
- There will be service interruptions on regular flights during the circulation of the directional buses
- All directional buses will be disinfected before departure, in the bus round belonging to the district, where this work is performed professionally by the district hygienists.
- With two escorts per bus, who disinfects the handrails in a short time before each round (everything that passengers are accomplished by hand)
- The attendant supervises them (keeping distance, wearing a mask, etc.) on the road, on the bus to avoid infection
- If the Vulnerable Population member can only travel by elevator, it is advisable for the attendant to get on the elevator and professionally bring them down to the bus waiting at the entrance. Do not touch anything in the in the elevator (6.9)
- For this reason, two attendants are needed, but this can be solved because those who supervise the outdoor activities are involved in the running on site among the elderly
Table A.5. Arrangement in buses. The average number of seats on an average bus is 30. The following arrangement can transport 23 people and ensure adequate spacing. The order of boarding, first saturation from the rear seats, is the opposite when disembarking. The optimal route determines the seating order.
| rows in the buses | bus / person two-thirds couples’ side by side, one-third alone total: 23 people |
|
| 1 | 2 | |
| 2 | 1 | |
| 3 | 1 | |
| 4 | 2 | |
| 5 | 2 | |
| 6 | 1 | |
| 7 | 1 | |
| 8 | 2 | |
| 9 | 2 | |
| 10 | 1 | |
| 11 | 1 | |
| 12 | 2 | |
| 13 | 2 | |
| 14 | 1 | |
| 15 | 1 | |
| Sum | 12 | 11 |
Table A.6. Optimal use of buses depending on the number of passengers to be transported to the districts. The load on buses can be reduced by (a) a certain number of patients entering the outdoor quarantine on a controlled footing, (b) if a certain number of patients use the bus every six days or twelve days instead of three. The six or twelve days will mainly be related those, who are living in a detached house with garden.
| Factors reducing bus congestion | Total number of passengers per district | Number of buses * | Total bus round | No of buses | No of round/ one bus | Travel time of one round in minutes | Total time per bus in minutes | Total time per bus per hour |
| 250,0 | 23,0 | 10,9 | 5,0 | 2,2 | 60,0 | 130,4 | 2,2 | |
| 50 people reach the area on foot in a controlled manner | 200,0 | 23,0 | 8,7 | 5,0 | 1,7 | 60,0 | 104,3 | 1,7 |
| 100 every six days for 50 people decrease / day | 150,0 | 23,0 | 6,5 | 5,0 | 1,3 | 40,0 | 52,2 | 0,9 |
| 100 every twelve days for 100 people decrease / day | 100,0 | 23,0 | 4,3 | 5,0 | 0,9 | 40,0 | 34,8 | 0,6 |
| 200 every twelve days for 200 people decrease / day | 50,0 | 23,0 | 2,2 | 5,0 | 0,4 | 40,0 | 17,4 | 0,3 |
| 350,0 | 23,0 | 15,2 | 10,0 | 1,5 | 60,0 | 91,3 | 1,5 | |
| 70 people reach the area on foot in a controlled manner | 280,0 | 23,0 | 12,2 | 10,0 | 1,2 | 60,0 | 73,0 | 1,2 |
| 100 every six days for 50 people decrease / day | 230,0 | 23,0 | 10,0 | 5,0 | 2,0 | 40,0 | 80,0 | 1,3 |
| 100 every twelve days for 100 people decrease / day | 180,0 | 23,0 | 7,8 | 5,0 | 1,6 | 40,0 | 62,6 | 1,0 |
| 200 every twelve days for 200 people decrease / day | 80 | 23,0 | 3,5 | 5,0 | 0,7 | 40,0 | 27,8 | 0,5 |
| 500,0 | 23,0 | 21,7 | 10,0 | 2,2 | 60,0 | 130,4 | 2,2 | |
| 100 people reach the area on foot in a controlled manner | 400,0 | 23,0 | 17,4 | 10,0 | 1,7 | 60,0 | 104,3 | 1,7 |
| 100 every six days for 50 people decrease / day | 350,0 | 23,0 | 15,2 | 5,0 | 3,0 | 40,0 | 121,7 | 2,0 |
| 100 every twelve days for 100 people decrease / day | 300,0 | 23,0 | 13,0 | 5,0 | 2,6 | 40,0 | 104,3 | 1,7 |
| 200 every twelve days for 200 people decrease / day | 200 | 23,0 | 8,7 | 5,0 | 1,7 | 40,0 | 69,6 | 1,2 |
The guidance for LTCF and chronic hospital departments (as it is introduced by the author in the Szent Donat hospital elderly/chronicle department including 300 patients. (https://www.raczt.hu/
- The patient should only be admitted after a negative Covid-19 test
- Each patient should be placed in a separate isolated ward, from which they should not move out for the next five days.
- On day 5, in the event of a negative test, they will be transferred to a four-bed ward, not to their final location. Here, too, it is not possible to leave the room for another 9 days (a total of 14) and after that it will be placed in its final place in case of another negative test.
- The single and quadruple wards are located on separate levels from the rest wards of the hospital.
- In the 300-bed chronic care ward, it is sufficient to provide 5-7 wards for the first five days for normal turnover.
- Once from here to a 4-5 bed ward, from where they are usually taken to a 1-2-3 bed final ward after 9 days, the 4-5 bed wards buffer the patient flow sufficiently to avoid congestion.
- These wards include dedicated nurses who do not have contact with the rest of the hospital.
- Single and childless nurses have been selected to supervise quarantine patient rooms.
- All nurses received special training to avoid viral contact. The hospital operated a separate minibus for those who did not have their own car to avoid public transport. The hospital’s technical staff arranged the purchases to meet the personal needs of the nurses and their families to avoid visiting the store. The hospital provided the nurses ’children with day care within the hospital, also to avoid potential infection. Patients should be tested every five days if possible.
- No infection occurred during the first wave, which was obviously greatly influenced by the series of effective measures that were introduced in Hungary.
The staff should be alerted for some specific symptoms that can be the sign of infection. Older people, living with co-morbidities react with reduced alertness and mobility, or diarrhea without fever.
If an infection occurs, in hotels and LTCF
- The special mobile military unit is withdrawn take over the operation.
- The necessary members of the former staff assist in their work in isolation.
- Everyone HQ, test and cannot go out the room for 14 days either.
Scenário
The essential elements are summarized in the following phases:
I. PHASE:
According to Grade I. (3.8.2.) Initially, we will focus our attention on those who voluntarily joined. Communication without coercive power continue. We would like to note an option with which we could defend them in a professional manner. In the same way, they can also rescue other’s lives, contributing to avoid overloading the capacity. This opportunity is strictly supervised. The VP thus determined must be provided with opportunities during the quarantine period to minimize discomfort. In cases of VCRH this is natural. Therefore, in th VPD, it is particularly important that the milieu creates a more comfortable and a rich framework of Spring "picnic" atmosphere and a more pleasant lifestyle, even as it was before in the VPDistricts even in wintertime. This picnic obviously means a geographically limited and possibly soldiers guarding zones. In addition, all volunteers will plug significant pension supplement. All of these are sufficiently motivated volunteering.
I. 0-7 days:
Preparatory work
- By the instructions of the CDC, Tessy, in UK, Germany, Hungary, Sweden (The National Authorities) through to the local-regional Professional Comittee and finally to the Family doctors (GPs) start identifying candidates for the Vulnerable population.
- The detecting and measuring of the VPCRH and the area of the VPD where potential outdoor activities can take place.
- The start of the mainstream and local media communication.
- Once you have a list of general practitioners, the directly walking residences, who lives in the proximity of districts should be compared with outdoor routes. In particular, the routes should be designed accordingly. Obviously, many borderline cases will be around the path, if the future capacity of the districts can be pressured.
II. Day 8-15:
Speed up the preparatory work.
- The organizers will draw up a plan for the feasibility, logistics, and assess the capacity of VPCRH and open spaces by the number of the Vulnerable population for each district is specified on the basis of a list finalized by GPs on the basis of the Selection Criteria Parameter score and other professional system.
- In each district, - if the capacity compromised - cases that are easier and more secure to deal with are given priority. (eg if a person lives in the open space next door, but a score equal to or below is of little value compared to those candidates whose transport is difficult, then - in agreement with the family doctor – make a decisions.)
- Routes to outdoor locations should be designated. It is necessary to establish the posts where you can control the movement of those VP who are walking to the district.
III. Day 15-19:
Strengthen communication, make contact with the Volunteers, where you can start uploading VPCRH and VPDistricts.
- Visiting and informing the candidates and relatives of the voluntary VP, signing declarations and commitments.
- In this phase, the Military Forces will take a more active role, placing cameras the forecourts of the entrances, housing exits of the Vulnerable Population. This is extremely necessary because, on the one hand, this method can be used to provide supervisory surveillance, field monitoring, and on the other hand, the elderly need as many signals as possible to identify themselves with the appropriate self-disciplinary attitude that adapts to the severity of the situation.
- In outdoor districts, it is advisable to check pre-positioned, (6 x 6 meters) fixed assets according to the needs.
- In the same way, check the hygienic conditions of the equipment and the quantity required (washbasins, hand basins, benches, tables, umbrellas, board games).
- Similarly, a systematic check of the current organization of the kitchen, catering place, transport and route with regard to the exclusion of the minimal possibility of infection.
- Organization of Masses (confession), place of preaching, pulpit, etc. Adherence to contact distance. For the sacrificial ceremony, the priest t must follow hygienic regulations. Priest will be tested before ceremonies. Immediate hand disinfection checked by professional soldier staff immediately before mass. Immediately before sacrifice or wearing another spectacular hand wash or professional staff to impress believers for pedagogical purposes. The wafer can only transfer between hands!
- The evacuating of VPDs starts.
II. PHASE:
If necessary, Grade II. (3.8.2) After the volunteers you can see how much capacity is available and how much they are being filled. We will launch another, more active, general and personalized campaign. The rest of the Vulnerable Population, in addition to mass communication, will be convinced to join the VPCRH and VPDistrict by trained communication professionals.
IV. 19-24days
Continue to fill places with Volunteers. Assess and compare the excess capacity of the with the number of GPs. If excess capacity exists, designation of additional non-voluntary but Vulnerable Population patients. Introducing Grade II (3.8.2) !
- Check the future movement of pedestrians. The transport vehicles check the delivery time with test roads. Here, proper logistics saves military personnel, and the assembly procedure becomes smoother to the “Picnic”.
- Develop the area with distance (6-6 m) programs.
V. 24-31 days
Visiting and persuading additional non-voluntary but Vulnerable Population candidates. It should involve previously well-prepared, professionally communicating experts with good persuasivene. Communication should rumble, should come from every media! The first Cruises and Resorts are start and turn to the maintenance period.
- Fine-tune districts.
- Due to the closing of the theater, the actors can rehearse and perform on the podiums set up outside the district. The theater season is about to begin.
- Other outdoor activities, worksheets, bingo, chess, etc.
VI. 28-31 days
Complete filling of districts with voluntary Vulnerable Population candidates. Urging the remaining patients over the age of 65 to adhere to the regulation as strictly as possible. Especially if they are struggling with two or more comorbidities. National summary of experiences.
III. PHASE:
When necessary start Grade III. Gradually all restrictions will be lifted the and life returns to its usual bed with full vehemence.
Necessary instructions for the ELSE Groups in order to avoid infection
For VPHQSB members:
Military control units have a mobile control device that can be used to identify them for certification. All members are required to carry their ID.
There is regular monitoring via the mobile. If they want to go out, they have to sign up and a soldier patrol sometimes goes there to chat, sharing news with them.
The several new kinds of apps should apply that senses when and where they moves out.
For VP District, VPHQSB, and (EM)HQBS members the protocol for receiving food or shipment is to:
(1) put on rubber gloves in the room (2) exit the door and disinfect the outer (!) handle, if by accidently would touch it after discarding the rubber gloves (3) open the velcro or outer remove the lid of the food container or other consignment container (4) discard the rubber glove in the outside bin and (5) take out the virus-free inner food container that you bring into the room, without gloves and begin to eat. After eating (6) pull rubber gloves again and (7) replace the inner food container to the outer food container. Close if necessary, the outer lid (8) with the second glove on it before going back through the open door, taking care not to touch the outer handle, (9) drop the rubber glove outside and go in, then close the door with the inner handle
For VPHQSB and EMHQBSWSDO members the protocol for going outside:
(1) The lift may only be entered dressed in rubber gloves, masks, and protective helmets. (2) The rubber glove should be discarded immediately upon reaching the open air, as the person occasionally touches his mouth and nose from time to time. They then need to refrain from touching anything. (3) The main rule of staying outdoors is to keep a distance, not only with strangers, but also especially with relatives. (4) A new rubber glove must be taken back in front of the elevator, which must be dropped into the biohazard box outside after opening the door before entering. (5) The boxes are sometimes taken away by soldiers. (6) Lifts, if possible, shall be fitted with a button indicating at each level that other occupants will not enter the lifts for as long as the signal lasts.
{kind=link}
{kind=link}